스테로이드는 급성 질환과 만성 질환 모두에서 광범위하게 사용되는 약물이다.
초생리적인 용량(sypraphysiological dose)에서 pro-inflammatory cytokine, T cell 기능 등을 억제하여 항염증 작용 & 면역 억제 효과를 나타낸다.
이러한 유효성에도 불구하고 다양한 부작용을 나타낸다.
| Immediate effect | fluid retention, blurred vision mood change, insomnia weight gain modulation of the immune response |
| Gradual effect | endocrine metabolism과 연관됨 hyperglycemia, central obesity, adrenal suppression, osteopenia→osteoporosis, dyslipidemia, acne, skin thinning dyspepsia(소화불량) |
| Idiosyncratic effect | avascular necrosis(무혈관성 괴사) cataract(백내장), open angle glaucoma(개방각 녹내장) psychosis |
특히 steroid induced hyperglycemia는 당뇨 환자뿐만 아니라 치료 전에는 당뇨 병력이 없었던 환자에서도 고혈당을 유발한다. 고혈당 발병률은 steroid 치료 환자의 약 46%이며, 기저 혈당의 68%까지 상승시킨다고 알려져 있다.
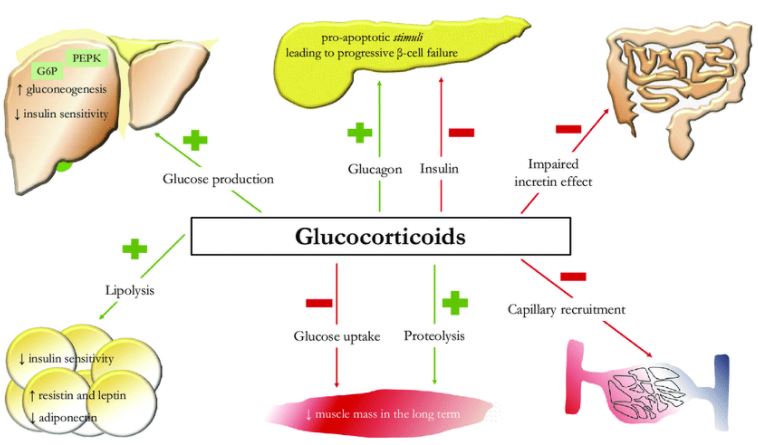
병태생리(Pathophysiology)
- 내인성 포도당 생성을 증가(glyconeogenesis)
- 인슐린의 작용 억제(antagonizing)
- 글루카곤, 에피네프린과 같은 counterregulatory hormone 작용 증강 → 내인성 포도당 합성 증가
- steroid induced nuclear receptor peroxisome proliferator-activated receptor α(PPAR-α)는 내인성 포도당 합성에 필수적임
- 근육세포와 지방세포에서 말초 포도당 재흡수를 억제시킴
- 췌장의 β 세포에서 인슐린의 분비와 생성을 억제
🍓 췌장의 β 세포에서 인슐린의 분비와 생성을 억제 & 포도당 생성을 증가 → 인슐린 저항성 증가

약물동태학(Pharmacokinetic) & 약물동력학(Pharmacodynamic)
| 합성 | adrenal |
| 분비 | circadian pattern & pulsatile ultradian rhythm |
| 정상 분비 범위 | 8-15 mg/day |
| 분포 | 10% : free form 90% (나머지) : 단백결합 (주로 albumin, cortisol binding globulin) |
| 반감기 | 혈장 반감기 : 80-270 min 작용 반감기 (조직 반감기) : 8-12 hr |
| 대사 | 간 대사 |
| 제거 | conjugated metabolite는 주로 신배설됨 |
인슐린 저항성은 주로 postprandial(식후)에 발생하며 스테로이드 종류에 따라 다양한 양상으로 나타난다.
| 지속성 | 성분명 | 특징 |
| intermediate acting | prednisone methylprednisolone |
peak of action : 4-6 hr |
| long acting | dexamethasone | hyperglycemia가 24시간 이상 지속됨 |
- 일반적으로 이러한 효과는 일시적이고 가역적이다. 스테로이드의 감량 시, 이러한 내분비적 대사 관련 효과는 정상으로 돌아오고 drug induced diabetes는 호전될 것이라 예상된다.
- 하지만 모든 케이스에서 그렇지만은 않았다. 장기간 스테로이드 사용 시 췌장 기능의 변화와 그로 인한 당뇨 발병에 대한 연구는 거의 없다. 최근 발표된 데이터에 따르면 스테로이드의 급성 투여 시, 특히 2-4주 동안 가장 큰 영향을 줄 수 있으며, 적응 현상(phenomenon of adaptation)으로 혈당은 자발적으로 완화된다고 한다.
<실제 steroid induced hyperglycemia 예>
아래 표는 실제 임상에서 ADR이 의심된 환자의 BST 모니터링 결과이다.
환자는 continuous EN feeding 중이며 칼로리는 1500-1700 kcal였다.
| BST monitoring 시각 | 07:00 | 11:00 | 17:00 | 22:00 |
| methylprednisolone 투여 전 |
137 | 160 | 170 | 147 |
| 150 | 138 | 157 | - | |
| methylprednisolone 투여 후(09:00 투약) |
152 | 168 | 234 | 206 |
| 123 | 139 | 181 | 123 |
진단
GC(glucocorticoid)-induced hyperglycemia의 진단은 미국 당뇨병 협회가 정한 기준과 유사하다.
- blood glucose level of ≥ 126 mg/dL
- glycemia at any time ≥ 200 mg/dL
- HbA1c > 6.5%
- blood glucose > 200 mg/dL 2 h after an oral glucose load
하지만 GC-induced hyperglycemia의 병태생리 패턴을 이해한다면 위의 진단 기준은 과소평가될 것으로 예상된다. 뿐만 아니라 두 가지 연구를 통해 실제 과소 평가 가능성을 보여주었다. (만성 스테로이드를 복용하는 신장 및 신경 질환이 있는 환자들의 식후 혈당은 > 200 mg/dL, 공복 혈당은 < 100 mg/dL로 관측됨)
GC-induced hyperglycemia는 주로 식후 상태에서 발생하기 때문에 fasting glucose를 이용하는 것은 물론 glucose tolerance curve 이용법을 권장하지 않는다.
뿐만 아니라 이식 환자의 경우, 면역억제제의 부작용 중 하나가 고혈당이기 때문에 이러한 환자군에서는 HbA1c 검사가 더 선호된다.
이전 연구들을 바탕으로 GD-induced hyperglycemia 평가를 위해서 다음의 검사법을 더 권장한다.
- 식후 혈당 검사 (intermediate acting GC의 경우 4-6 hr 후의 식후 혈당 검사가 권장됨)
- HbA1c 검사
입원 환자의 모니터링
- 스테로이드 치료 시작 전 BST 체크
- 병원 환경에서 스테로이드 치료 개시 후 1-2 일 이내 발생함
- 24-48 시간 동안 인슐린 요구없이 BST가 140 mg/dL 이하로 유지되는 경우, 비당뇨환자의 BST monitoring을 중단할 수 있음
- 140 mg/dL 초과하는 경우 insulin SC를 통해 혈당 조절을 시작
- insulin SC로도 혈당 조절이 되지 않는 경우, infusion pump(continuous infusion)를 이용한 혈당 조절이 필요함
cf) GC-induced hyperglycemia의 위험도 평가를 위한 프로토콜 존재 (유용성 확인을 위한 추가 연구가 필요함)[2]
- 가설 : pre-diabetic 환자의 인슐린 분비 이상/베타세포 기능 상실 → GC exposure 이후 → 인슐린 요구량 증가
- sterr test : 8 mg dexamethasone 투여 → 혈당/C-peptide/insuline의 증가를 관측
reference:
1) Tamez-Pérez, Héctor Eloy, et al. "Steroid hyperglycemia: Prevalence, early detection and therapeutic recommendations: A narrative review." World journal of diabetes 6.8 (2015): 1073.
2) Abdelmannan, Dima, et al. "Effect of dexamethasone on oral glucose tolerance in healthy adults." Endocrine Practice 16.5 (2010): 770-777.
3) Bonaventura, Aldo, and Fabrizio Montecucco. "Steroid-induced hyperglycemia: an underdiagnosed problem or clinical inertia? A narrative review." Diabetes research and clinical practice 139 (2018): 203-220.
'🤹♂️ 카테고리별 약물 > 내분비' 카테고리의 다른 글
| steroid induced hyperglycemia, 스테로이드 유발 고혈당, steroid-induced diabetes mellitus (SIDM)(3) (0) | 2021.01.21 |
|---|---|
| steroid induced hyperglycemia, 스테로이드 유발 고혈당, steroid-induced diabetes mellitus (SIDM)(2) (0) | 2021.01.20 |
| corticosteroid tapering 기간, 방법 (0) | 2021.01.03 |
| steroid, cortisol, corticosteroid equivalnet (0) | 2021.01.02 |
| Clinical Use of DPP-4 Inhibitors, DPP-4 inhibitor 비교 (0) | 2020.11.06 |

댓글