
정맥혈전증(Venous tromboembolism, VTE)
- injury, surgery, and critical illness이 위험 요인이다.
- 외상 중환자에서는 환자의 VTE 위험 요인을 평가하고 기계적 및 약물학적 예방 조치 사용을 매일 논의하여야 한다.
- Trauma and surgical patients often have real or perceived contraindications to prophylaxis that affect the timing of preventive measures and the consistency with which they can be applied.
- In this Clinical Consensus Document, the American Association for the Surgery of Trauma Critical Care Committee addresses several practical clinical questions pertaining to specific or unique aspects of VTE prophylaxis in critically ill and injured patients.
- The goal of these documents is to provide practical answers to common clinical questions based on the best evidence available.
- They address focused topics for which the levels of evidence guiding care may not be strong and/or practice is controversial, and are based on expert consensus and review of the literature.
- Venous thromboembolism (VTE) prophylaxis, emphasizing the intensive care unit (ICU) environment, was chosen by the Committee as an area of practice warranting review and consensus.
TBI(traumatic brain injury)
1. When should chemical VTE prophylaxis be initiated after TBI?
- 정맥혈전증 예방은 외상성 뇌손상 이후 가능한 빨리 시작되어 출혈 부위 확장과 VTE의 위험의 균형을 맞춰야 한다.
- 사용가능한 문헌에서는 입원 후 24-72시간 이내 시작하는 것을 권고하고 있음. 하지만 intracranial/extracranial hemorrhage가 있을 때 신경외과 협진까지 연기해야 한다.
- Early (<72 hours) versus late (>72 hours) prophylaxis in severe TBI, showing lower rates of pulmonary embolus (PE) and deep vein thrombosis (DVT) in the early group without subsequent increases in neurosurgical intervention or mortality. [J Am Coll Surg. 2016 Oct; 223(4):621-631.e5.]
- 단일 기관 후향적 연구에서 중증의 외상성 뇌손상 환자에게서 VTE 예방 요법의 시간에 따라 4가지 그룹으로 나눔: <24 hours, 24–48 hours, >48 hours, no therapy. early (<24 hours) administration군에서 ICH의 진행과는 연관 없었다. [World J Surg. 2019 Nov; 43(11):2804-2811.] VTE 예방 요법에 따른 ICH 진행의 전체 발병률은 문헌적 발병률에 비해 높은 편이지만 한 코호트 연구에 비해서는 낮았다.[Neurosurgery 2017;81:1016–20.]
2. Should severity of TBI influence timing and dosage of chemoprophylaxis?
- 예방 요법의 시작 시기는 개별화 필요함
- Categorized as BIG 1–3, only patients meeting BIG 3 criteria (>8 mm ICH) required neurosurgical intervention. Furthermore, the Berne-Norwood criteria suggest that, in the absence of multiple contusions, for isolated subarachnoid/intraventricular hemorrhage and subdural/epidural ≤8 mm prophylaxis may safely be initiated at 24 hours postinjury pending stability of head CT.
- moderate-risk and high-risk group으로 계층화하여 VTE 예방이나 inferior vena cava(IVC)는 72시간까지 지연될 수 있다.
- 일반적으로 enoxaparin 30 mg bid or UFH 5,000 IU tid으로 가장 흔하게 투여된다.
- 특히나 LMWH의 경우, anti Xa분석을 통한 평가로 ICH 진행의 위험 증가없이 목표 범위 내에서 평가할 수 있다.
3. Is there a preferred chemoprophylaxis agent for patients with TBI?
- LMWH (superior) > UFH
- Current recommendations from the BTF support either UFH or LMWH for VTE prophylaxis and cannot conclusively endorse superiority of either, leaving room for future prospective studies [Brain Trauma Foundation . Guidelines for the Management of Severe TBI, 4th Ed]
- 더 짧은 반감기의 이론적 이점 때문에 일부에서는 UFH의 TBI 고용을 선호할 수 있다.
- LMWH의 사용은 1일 1회 요법이라는 점에서 환자의 거부감 감소와 같은 몇 가지 실질적인 이점을 UFH보다 제공할 수 있다.
- aspirin이나 NOAC을 이용한 VTE 예방 대안법이 연구 중에 있으며 그 중 aspirin은 대규모 RCT가 진행중임. 두 가지 방법 모두 추가 연구가 필요하며 공식화할 증거가 불충분하다.
Solid organ injury
1. What timing and agent is appropriate for VTE prophylaxis after blunt solid organ injury?
- In patients with blunt solid organ injury (SOI) undergoing non-operative management, 지속적인 출혈 또는 다른 금기가 없는 경우, VTE prophylaxis with LMWH는 48시간 이내 시행
- 간, 신장, 비장 등의 장기에 blunt injury를 입은 환자의 경우, non-operatively 관리를 받을 가능성이 높으며 이는 VTE prophylaxis를 시작하기에 안전한 환자군이 될 것이다.
- 지혈이 완료된 이후, 예방적 요법은 가능한 빨리 시작되는 것이 좋다. 한 후향적 연구에서 thromboelastography (TEG) parameter를 이용하여 blunt 고형 장기 손상을 받은 환자군에서 손상 약 48시간 이후 hypercoagulable state가 진행됨이 관찰되었고 이는 VTE 예방요법의 시작 시간의 중요성을 시사했다.
- 고형 장기 손상의 VTE 예방 시점을 비교하는 RCT는 없지만 여러 관찰 연구(observational study)가 있다. early (typically <48 hours after injury) vs. late (>48 hours after injury) initiation. 일괄적으로 각 연구에서 transfusion requirements or failure of non-operative management requiring intervention의 증가는 관찰되지 않았다.
- UFH이나 LMWH 중 superiority를 비교한 high-quality data or consensus는 없지만 다발외상성 환자에서 LMWH를 더 선호하므로 이를 우선 권장하는 바이다.
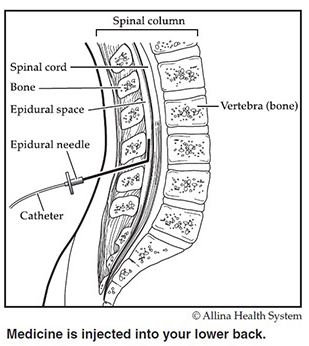
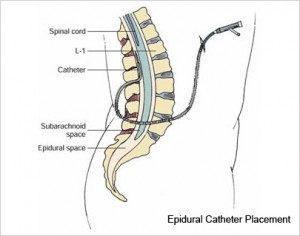
Epidural analgesia
1. Should trauma patients with epidural catheters receive pharmacological prophylaxis and, if so, which agent and at what dose?
- Epidural catheter가 있는 외상 환자에서 enoxaparin을 받을 때 epidural catheter가 없는 환자와 비슷한 용량을 투여한다. 신부전 환자의 경우 UFH를 선호한다.
- Epidural catheter 삽입 후, enoxaparin이 중단되는 경우가 많으며 이는 VTE 비율을 증가시켰다.
- Regional anesthesia guidelines에서 enoxaparin 투여와 epidural catheter 삽입 혹은 제거 사이 12시간 간격(표준 투여량보다 고용량인 경우 24시간)을 권고하며 약물의 재개(restart)는 4-12시간 간격을 권장한다.
- UFH의 경우 catheter 삽입 또는 제거시 약물 투여 사이의 간격을 4-6시간으로 단축할 수 있으며, 약물의 재개는 1시간 간격으로도 충분하다. 따라서 UFH는 중단할 필요가 없다.

reference:
1) Rappold, Joseph F., et al. "Venous thromboembolism prophylaxis in the trauma intensive care unit: an American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document." Trauma Surgery & Acute Care Open 6.1 (2021): e000643.
2) wikipedia
3) https://www.allinahealth.org
4) https://www.rushpaincenter.com/
728x90
'🤹♂️ 카테고리별 약물 > 심혈관' 카테고리의 다른 글
| 스트레스성 심근병증(stress induced cardiomyopathy; SCMP), Takotsubo cardiomyopathy의 치료 (1) | 2021.06.12 |
|---|---|
| VTE(정맥혈전증) LMWH, Enoxaparin monitoring: anti-Xa, viscoelastic monitoring (0) | 2021.05.15 |
| PO amiodarone vs IV amiodarone: 투여 경로에 따른 약리 작용(기전), 부작용 차이 (0) | 2021.04.11 |
| Fluoroquinolone계 항생제의 QT연장 심혈관계 부작용 (0) | 2021.04.11 |
| Statin(콜레스테롤 저하제) 약제 투여 시간, 저녁 복용 vs 아침 복용 (1) | 2021.04.06 |

댓글