국내허가사항에서는 프레세덱스 주(dexmedetomidine)의 용법 용량을 다음과 같이 기술하고 있다.

그 밖의 사용상의 주의사항을 살펴보면 다음과 같다.
집중치료 관리하의 진정에서 사용 시 유지용량은 0.7μg/kg/hr을 초과하여 사용하지 않는다. (해외 임상 연구 중 장기 사용 시 투여 농도가 0.7μg/kg/hr을 넘을 경우 호흡기계, 정신신경계 및 심혈관계 부작용이 증가한다는 보고가 있다.)

하지만 연구가 진행됨에 따라 해당 최대 용량보다 더 고용량 사용에 대해 고려해봐야 한다. 오늘은 0.7 mcg/kg/hr 이상의 용량에 대한 safety와 efficacy에 대해 알아보고자 한다.
(1) MENDS trial; Jama 298.22 (2007): 2644-2653.
Context
Lorazepam*은 MV(mechanically ventilator)받는 환자에서 진정 유지를 위해 권장되고 있지만 lorazepam을 포함한 다른 benzodiazepine(BZD)계열 약물은 경우 급성 뇌 부전(delirium and coma 등)을 유발할 수 있으며 이는 재원 기간과 병원비, 사망률을 증가시킨다. dexmedetomidine의 경우 BZD와는 다른 central nervous system의 수용체를 통한 진정을 유도하기 때문에 급성 뇌 부전의 위험이 감소될 수 있다.
*Crit Care Med. 2002;30(1):119-14111902253
Objective
To determine whether dexmedetomidine reduces the duration of delirium and coma in mechanically ventilated ICU patients while providing adequate sedation as compared with lorazepam.
Design, Setting, Patients, and Intervention
Double-blind, randomized controlled trial
between August 2004 and April 2006
106 adult mechanically ventilated medical and surgical ICU patient
| Lorazepam | Dexmedetomidine | |
| final concentration | 1 mg/mL | 0.15 μg/kg per mL |
| start rate | 1 mg/h | 0.15 μg/kg per hour |
| maximum rate | 10 mg/h | 1.5 μg/kg per hour |
블라인드 상황을 유지하고 잠재적인 부작용을 최소화하는 bolus 대신 infusion 방법을 사용하였다. (dexmedetomidine의 rapid bolus로 인해 hypotention/bradycardia 유발 위험)
sedative의 시작은 1 mL/h → maximum of 10 mL/h
120 hr*동안 각각의 진정제를 투여받음
*FDA에서 허가받은 최대 시간
Fentanyl: Apparent pain에 따라 intermittent dose of fentanyl이 투여되었고 뿐만 아니라 10 mL/h로도 충분한 sedation에 도달하지 못하였을 때도 intermitten dose of fentanyl이 투여되었다.
Propofol: 갑작스럽고 위급한 수준의 섬망/동요 발생 시 25-50 mg의 propofol bolus가 투여되었다.
Richmond Agitation-Sedation Scale (RASS)을 이용하여 목표 진정 수준에 달성
the Confusion Assessment Method for the ICU (CAM-ICU).을 하루 2회 평가하여 섬망 모니터링
Main Outcome Measures
Days alive without delirium or coma and percentage of days spent within 1 RASS point of the sedation goal.
Results

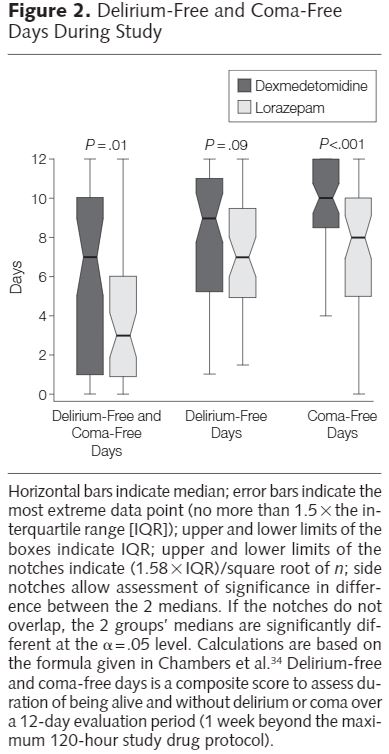



Conclusion
The MENDS trial 결과로 중증 환자에서 dexmedetomidine 사용에 관한 추가적인 안전성 데이터가 추가되었다.
이 연구에서 dexmedetomidine은 FDA 승인된 용량의 2배과 사용 기간의 5배에 달하는 용법/용량으로 수행되었다. (We accomplished this through working within the context of an FDA Investigational New Drug approval for this study, thereby allowing us to test dexmedetomidine at as much as twice the approved maximum dose and as much as 5 times longer than the currently approved, yet impractical and limiting, 24-hour infusion period.)
특히 volume-depleted patients에서 hypotension을 유발하였지만 이번 연구에서는 두 군에서 모두 관찰되었다. sinus bradycardia의 경우, dexmedetomidine군에 더 빈번하였지만 각 군에서 오직 1명씩만 glycopyrolate 치료를 받았다.
dexmedetomidine는 lorazepam과 반대로 진통 효과가 있는 것으로 알려졌지만 fentanyl의 사용량은 dexmedetomidine군이 더 많았다. 이는 혼수 상태에 빠지는 시간이 더 적었기 때문에 간호사에게 진통의 필요성이 더 잘 전달되었을 가능성이 있다. 또한 fentanyl의 진정 특성 때문에 dexmedetomidine군에서 깊은 진정 시 영향을 끼쳤을 가능성이 있다고 생각된다.
(2) SEDCOM trial; Jama 301.5 (2009): 489-499.
Context
γ-Aminobutyric acid receptor agonist medications are the most commonly used sedatives for intensive care unit (ICU) patients, yet preliminary evidence indicates that the α2 agonist dexmedetomidine may have distinct advantages.
Objective
To compare the efficacy and safety of prolonged sedation with dexmedetomidine vs midazolam for mechanically ventilated patients.
Design, Setting, and Patients
Prospective, double-blind, randomized trial conducted in 68 centers in 5 countries between March 2005 and August 2007 among 375 medical/surgical ICU patients with expected mechanical ventilation for more than 24 hours. Sedation level and delirium were assessed using the Richmond Agitation-Sedation Scale (RASS) and the Confusion Assessment Method for the ICU.
Interventions
| dexmedetomidine | midazolam | |
| mean (SD) maintenance infusion dose | 0.83 (0.37) μg/kg per hour | 0.056 (0.028) mg/kg per hour |
Dexmedetomidine (0.2-1.4 μg/kg per hour [n = 244]) or midazolam (0.02-0.1 mg/kg per hour [n = 122]) titrated to achieve light sedation (RASS scores between −2 and +1) from enrollment until extubation or 30 days.
Main Outcome
Measures Percentage of time within target RASS range. Secondary end points included prevalence and duration of delirium, use of fentanyl and open-label midazolam, and nursing assessments. Additional outcomes included duration of mechanical ventilation, ICU length of stay, and adverse events.
Results


Conclusions
환자의 61%에서 dexmedetomidine는 시간당 최대 용량인 0.7 mcg/kg/hr을 초과하였으며 환자의 80%는 승인된 24시간보다 더 오랫동안 투여 받았다.
이 연구에서 24시간 이상, 최대 1.4 mcg/kg/hr 투여 시, midazolam과 유사한 진정 효과를 제공하였으며 안전성과 섬망 개산과 관련이 있음을 확인했다.
dexmedetomidine군에서 bradycardia 발생률이 2배 더 높았던 반면 midazolam군에서는 tachycardia와 hypertention 발생률이 더 높았다. clonidine과 달리 dexmedetonidine 중단 후 48시간 추적기간 동안 rebound hypertension이나 tachycardia에 대한 근거는 검출되지 않았다.
(3) MIDEX/PRODEX trial; Jama 307.11 (2012): 1151-1160.
Context
장기간 midazolam과 propofol 사용 시 체내 축적이 예상된다. 뿐만 아니라 고선량/장기간 propofol 사용은 PRIS(propofol infusion syndrome)를 유발할 수 있다. 이에 dexmedetomide의 경우 장기간 사용에도 비교적 안정적이라고 예상된다.
Objective
dexmedetomidine이 midazolam이나 propofol보다 mild to moderate sedation을 유지하기에 적절한지 기계환기 기간이나 ICU 재원 기간을 감소시키는 이점이 있는지 알아보고자 한다.
Design, Setting, and Patients
Two phase 3 multicenter, randomized, double-blind trials carried out from 2007 to 2010. The MIDEX trial compared midazolam with dexmedetomidine in ICUs of 44 centers in 9 European countries; the PRODEX trial compared propofol with dexmedetomidine in 31 centers in 6 European countries and 2 centers in Russia. Included were adult ICU patients receiving mechanical ventilation who needed light to moderate sedation for more than 24 hours (midazolam, n = 251, vs dexmedetomidine, n = 249; propofol, n = 247, vs dexmedetomidine, n = 251).
Interventions
Sedation with dexmedetomidine, midazolam, or propofol; daily sedation stops; and spontaneous breathing trials.
| dexmedetomidine | midazolam | propofol |
| 0.2-1.4 μg/kg per hour | 0.03-0.2 mg/kg per hour | 0.3-4.0, mg/kg per hour |
Main Outcome
Measures For each trial, we tested whether dexmedetomidine was noninferior to control with respect to proportion of time at target sedation level (measured by Richmond Agitation-Sedation Scale) and superior to control with respect to duration of mechanical ventilation. Secondary end points were patients' ability to communicate pain (measured using a visual analogue scale [VAS]) and length of ICU stay. Time at target sedation was analyzed in per-protocol population (midazolam, n = 233, vs dexmedetomidine, n = 227; propofol, n = 214, vs dexmedetomidine, n = 223).
Results


Dexmedetomidine/midazolam ratio in time at target sedation was 1.07 (95% CI, 0.97-1.18) and dexmedetomidine/propofol, 1.00 (95% CI, 0.92-1.08). Median duration of mechanical ventilation appeared shorter with dexmedetomidine (123 hours [IQR, 67-337]) vs midazolam (164 hours [IQR, 92-380]; P = .03) but not with dexmedetomidine (97 hours [IQR, 45-257]) vs propofol (118 hours [IQR, 48-327]; P = .24). Patients' interaction (measured using VAS) was improved with dexmedetomidine (estimated score difference vs midazolam, 19.7 [95% CI, 15.2-24.2]; P < .001; and vs propofol, 11.2 [95% CI, 6.4-15.9]; P < .001). Length of ICU and hospital stay and mortality were similar. Dexmedetomidine vs midazolam patients had more hypotension (51/247 [20.6%] vs 29/250 [11.6%]; P = .007) and bradycardia (35/247 [14.2%] vs 13/250 [5.2%]; P < .001).
Conclusions
Among ICU patients receiving prolonged mechanical ventilation, dexmedetomidine was not inferior to midazolam and propofol in maintaining light to moderate sedation. Dexmedetomidine reduced duration of mechanical ventilation compared with midazolam and improved patients' ability to communicate pain compared with midazolam and propofol. More adverse effects were associated with dexmedetomidine.
이전 연구 결과를 토대로 dexmedetomidine은 deep sedation에 적합하지 않다는 것을 알 수 있었다. 따라서 이번 실험은 light-moderate sedation에 초점을 맞추었다.
최대 용령에서도 8-10명 당 1명꼴로 진정 효과가 부족함이 예상된다. 고선량에서 안전하게 사용될 수 있는지 여부는 향후 연구를 통해 다루어져야 한다.
진정 수준이 유사함에도 불구하고 dexmedetomidine 선량은 propofol vs dexmedetomidine 연구보다 midazolam vs dexmedetomidine에서 적었다. 이는 midazolam의 잔존 효과 때문일 가능성이 있다.
reference:
(1) Pandharipande, Pratik P., et al. "Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial." Jama 298.22 (2007): 2644-2653.
(2) Riker, Richard R., et al. "Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial." Jama 301.5 (2009): 489-499.
(3) Jakob, Stephan M., et al. "Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials." Jama 307.11 (2012): 1151-1160.
(4) Meyers, Bruce. "A Retrospective Review of High versus Standard Dose Dexmedetomidine for Sedation in Critically Ill Patients." Journal of Intensive and Critical Care 2.2 (2016): 16.
'🤹♂️ 카테고리별 약물 > 진통·진정' 카테고리의 다른 글
| IV PCA 안정성(stability): 언제까지 보관할 수 있을까? (0) | 2021.06.16 |
|---|---|
| 수술실 약제: 근이완제, 진정제, 진통제 (0) | 2021.06.05 |
| ARDS(acute respiratory distress syndrome) 치료: NMBA, sedative agent (0) | 2021.03.27 |
| NSAIDs계 소염진통제, COX-2 선택적 억제제, 진통제 (0) | 2021.02.28 |
| Vecuronium, long term administration, 베카론 주, 사용 기간 (0) | 2021.02.09 |

댓글