지주막하출혈(Subarachnoid Hemorrhage; SAH)
- 자발 또는 외상에 의하여 나타남, 가장 흔한 원인은 뇌동맥류(약 80%)임
- 지주막하출혈은 전체 뇌졸증의 약 5%를 차지함
- 빠른 수술 혹은 혈관 내 중재시술과 함께 1960년대 35%였던 사망률이 2000년대 20%로 감소됨
- 두개내압(intracranial pressure; ICP) 증가 또는 뇌관류압(cerebral perfusion pressure; CPP)의 감소는 나쁜 예후를 보임
- 조기 뇌동맥류 결찰 혹은 coiling한 후 주의해야할 합병증: 재출혈, 뇌혈관연축(cerebral vasospasm), 수두증(hydrocephalus), 저나트륨혈증, 지연 허혈성 신경학적 결손(delayed ischemic neurological deficits; DID) 등

1. 재출혈
- 24시간 이내 4%, 그 이후로 매일 1% 정도 발생 위험이 감소됨(출혈 24시간 이내 재출혈 위험이 가장 높음)
- 출혈 이후 14일 동안 누적 위험은 15-25% 정도임
- 사망률이 50-70%에 이르는 매우 심각한 합병증임
- SAH 발생 환자의 경우 안정화된 후 파열된 동맥류의 재출혈을 방지하는 것이 중요함
<Neurología (English Edition) 29.6 (2014): 353-370>

<Cerebrovascular diseases 35.2 (2013): 93-112>
- There is currently no medical treatment that improves outcome by reducing rebleeding (class I, level A)
- Results from some small trials that used haemostatic agents suggest further investigations with modified protocols (class II, level C)
① Intervention: clipping vs. coiling
| clipping | coiling |
| younger age, presence of space occupying ICH (class II, level B), and aneurysm-specific factors such as: – location: middle cerebral artery and pericallosal aneurysm (class III, level B) – wide aneurysm neck (class III, level B) – arterial branches exiting directly out of the aneurysmal sack (class III, level B) – other unfavourable vascular and aneurysmal configuration for coiling (class IV, level C) |
age above 70 years, (class II, level B), space occupying ICH not present (class II, level B), and aneurysm-specific factors such as: – posterior location – small aneurysm neck – unilobar shape (class III, level B). |
② Antifibrinolytic Treatment
| Tranexamic acid (CRASH-3 trial) |
부상 후 3시간 이내 1 g (in NS 100 mL) over 10 min ⇨ 1 g (in NS 500 mL) for 8 hr (100 mL NS or 5DW 희석) |
| ɛ-aminocaproic acid (국내 X) |
4 g (in NS 200 mL) over 15-60 min ⇨ 1 g/hr (최대 투여 기간 72 hr) |
| p-Aminomethyl Benzoic Acid | SAH에 대한 연구 없음 |

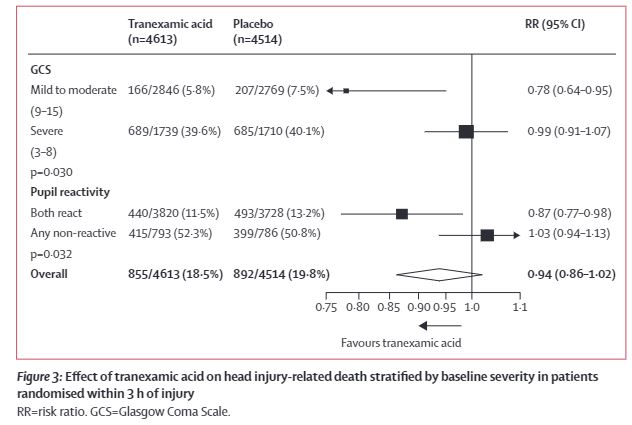
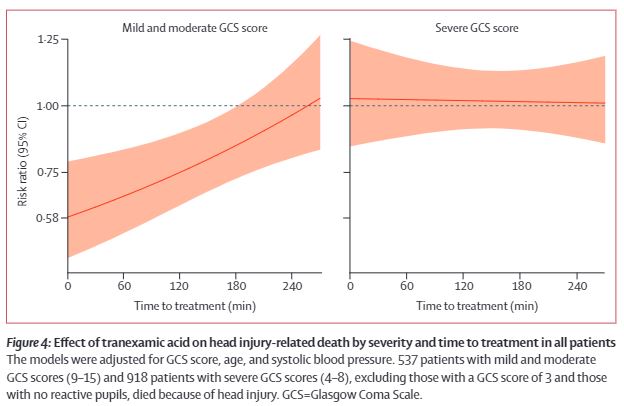
- Our results show that tranexamic acid is safe in patients with TBI and that treatment within 3 h of injury reduces head injury-related death. Patients should be treated as soon as possible after injury.
- 지혈제 사용으로 인한 DVT, PE, stroke 등의 부작용은 대조군과 치료군에서 유의한 차이를 보이지 않았음
③ Recombinant Factor VIIa
- 이론적으로 재출혈 예방이 가능함, 하지만 DVT 위험이 있음
- 현재 SAH 환자에 대한 사용을 뒷받침하는 근거는 없음
④ Antihypertensive treatment
- 혈압이 급상승하는 경우, 모니터링을 하고 짧은 반감기를 가지는 labetalol과 같은 항고혈압 약제를 고려할 수 있음
- SAH 후 고혈압 치료는 RCT 증거가 부족하기 때문에 논란이 됨
- Observational study에서 공격적인 혈압 조절로 인해 재출혈 위험은 낮출 수 있지만 2차성 허혈의 위험이 증가할 수 있음을 제안함
- ‘Extreme’ blood pressure 상태에서 고혈압 치료를 고려할 수 있으나 extreme의 정의하기 어렵고 개별화 해야한다는 어려움이 있음
- 동맥류가 교정되지 않은 경우 SBP 180 mmHg 이하 유지를 위해 짧은 반감기를 가지는 lebetalol, esmolol을 고려할 수 있음


reference:
1) Mees, Sanne Dorhout, et al. "Calcium antagonists for aneurysmal subarachnoid haemorrhage." Cochrane database of systematic reviews 3 (2007).
2) Carlson, Andrew P., et al. "Nimodipine reappraised: an old drug with a future." Current neuropharmacology 18.1 (2020): 65-82.
3)Kramer, Daniel R., et al. "Cortical spreading depolarization: pathophysiology, implications, and future directions." Journal of Clinical Neuroscience 24 (2016): 22-27.
4) 김규식. "지주막하출혈 환자에서 뇌혈관연축 치료의 현재와 미래." 대한신경집중치료학회지 3.1 (2010): 1-6.
5) Mees, Sanne M. Dorhout, et al. "Magnesium for aneurysmal subarachnoid haemorrhage (MASH-2): a randomised placebo-controlled trial." The Lancet 380.9836 (2012): 44-49.
6) Keyrouz, Salah G., and Michael N. Diringer. "Clinical review: Prevention and therapy of vasospasm in subarachnoid hemorrhage." Critical care 11.4 (2007): 1-10.
7) Connolly Jr, E. Sander, et al. "Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association." Stroke 43.6 (2012): 1711-1737.
8) Vivancos, J., et al. "Clinical management guidelines for subarachnoid haemorrhage. Diagnosis and treatment." Neurología (English Edition) 29.6 (2014): 353-370.
9) Steiner, Thorsten, et al. "European Stroke Organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage." Cerebrovascular diseases 35.2 (2013): 93-112.
10) CRASH, The. "Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial." The Lancet 394.10210 (2019): 1713-1723.
'🤹♂️ 카테고리별 약물 > 신경' 카테고리의 다른 글
| Haloperidol의 올바른 투여 (2탄): IV 투여는 금기인가? (0) | 2021.08.17 |
|---|---|
| Gabapentin(가바펜틴, 뉴론틴)의 신기능에 따른 용량 조절, CRRT 시 용량 (0) | 2021.08.05 |
| Phantom Limb Pain 관리: 환상지통(환상통), 절단(amputation) (0) | 2021.05.23 |
| 만성 알코올 중독자의 ICU management: agitation, baclofen (0) | 2021.05.12 |
| 항정신병약제(antipsychotic) 간 효능/부작용 차이 (0) | 2021.04.03 |

댓글