
후탄 주 10 mg의 허가사항의 용법 용량
- 췌염의 급성증상(급성췌염, 만성췌염의 급성 악화기, 수술후의 급성췌염, 췌관조영술 후의 급성췌염, 외상성 췌염)의 개선
- 파종혈관내응고증(DIC)
- 출혈성 병변 또는 출혈경향을 갖는 환자의 혈액체외순환시 관류혈액 응고방지(혈액투석 및 혈장분리반출술)
후탄 주 50 mg의 허가사항의 용법 용량
- 파종혈관내응고증(DIC)
- 출혈성 병변 또는 출혈경향을 갖는 환자의 혈액체외순환시 관류혈액 응고방지(혈액투석 및 혈장분리반출술)
**용량마다 허가사항 indication이 다르기 때문에 10 mg짜리로 50 mg 처방이 나는 이유다!
허가사항(췌장염)의 재구성/희석
| 방법 |
추천 |
| 재구성 |
10 mg당 1mL 이상의 5DW or SWI |
| 희석 | 500 mL 5DW |
허가사항의 투여방법
- acute pancreatitis : 10 mg nafamostat+ 5DW 500 mL (over 2 hr) bid
- DIC : 0.06∼0.20mg/kg/hr(=60 kg 기준 86.4-288 mg/day) + 5DW 1000 mL cont. infusion
- RRT시의 anticoagulation : to be continued...
** 용해 시의 주의 : 백탁 또는 결정이 석출 될 수 있으므로 생리식염액 및 무기염류를 함유한 용액을 바이알에 직접 가해서는 안된다. = NS를 재구성 용제로 사용하지 말 것! 뿐만 아니라 희석액도 웬만하면 DW로!
급성 췌장염(acute pancreatitis)이란?
- abdominal inflammatory disorder
- 췌장의 protease trypsin의 ectopic activation(활성화되야하는 부분 외에서 활성화됨), 트립신(trypsin)은 췌장 소화 효소의 순차적인 활성에 trigger 역할을 한다. acinar cell의 injury로 trypsin이 분비되면 pancreatic & peripancreatic necrosis 뿐만 아니라 organ failure까지 유발할 수 있다. (mainly as a result of vascular injury)
"그렇다면 트립신의 activation을 억제할 수 있는 protease inhibitor를 급성 췌장염에 사용할 수 있지 않을까?"
해서 탄생한 것이 nafamostat mesilate, gabexate mesilate이다.
그렇다면 정말 protease inhibitor가 효과가 있을까?
치료 성적은 기대에 미치지 못했다. 이는 약제가 효과를 발휘하기 위해서는 (1) early phase에 투여되어야 하며 (2) pancreatic perfusion 감소로 췌장에 충분한 농도로 도달하지 못한다는 점 때문이라고 생각된다.
하지만 실제 임상에서는 20 mg/day보다 고용량을 사용하는 것을 알 수 있다.
고용량 사용 시 췌장으로 고농도를 유지되어 치료효과가 더 좋을 것으로 예상된다. 정말 그러한지 2개의 study를 살펴보자.
고용량 nafamostat 연구(1)
[1] 다음은 post ERCP pancreatitis 예방을 위해 high dose nafamostat mesilate가 효과적인지에 대해 알아보는 연구이다.
N = 595 명의 ERCP를 진행한 환자
| control group (A) | 20 mg nafamostat (B) | 50 mg nafamostat (C) |
outcome :
- overal incidence of acute pancreatitis 7.4%(44/595)
- 각 nafamostat유무에 따른 incidence of PEP(post-ERCP pancreatitis)는 임상적으로 유의한 차이 O
(13.0% vs 4.0% / 5.1% 각각 P <0.0001)
- low risk patient에서 nafamostat 투여군에서 rate of PEP는 임상적으로 유의하게 감소됨
(11.9% vs 2.7% / 4.0% 각각 P=0.007)
- high risk pateint에서 nafamostat 투여군에서 rate of PEP는 임상적으로 차이가 없음
(14.6% vs 5.9% / 6.9% 각각 P= 0.108)
😁 결론 : post ERCP pancreatitis 예방을 위해 nafamostat를 사용하는 것은 효과적이지만 high risk patient 군에서 high dose nafamostat를 사용하는 것은 임상적으로 유의하게 효과적이지는 못하다.
고용량 nafamostat 연구(2)
[3] 다음은 2004년에 발표된 단백효소 저해제의 효과에 대한 meta 분석이다.
결과 : Treatment with protease inhibitors does not significantly reduce the mortality in patients with acute or mild pancreatitis, but may reduce the mortality in patients with moderate to severe pancreatitis.
고용량 gabexate 연구(3)
[4] 다음은 2014년에 발표된 [3] 논문 저자의 updated systematic review & meta analysis이다.
여러 논문에 의해 protease inhibitor의 IV 투여의 효과에 대해서는 여전히 controversial 하다.
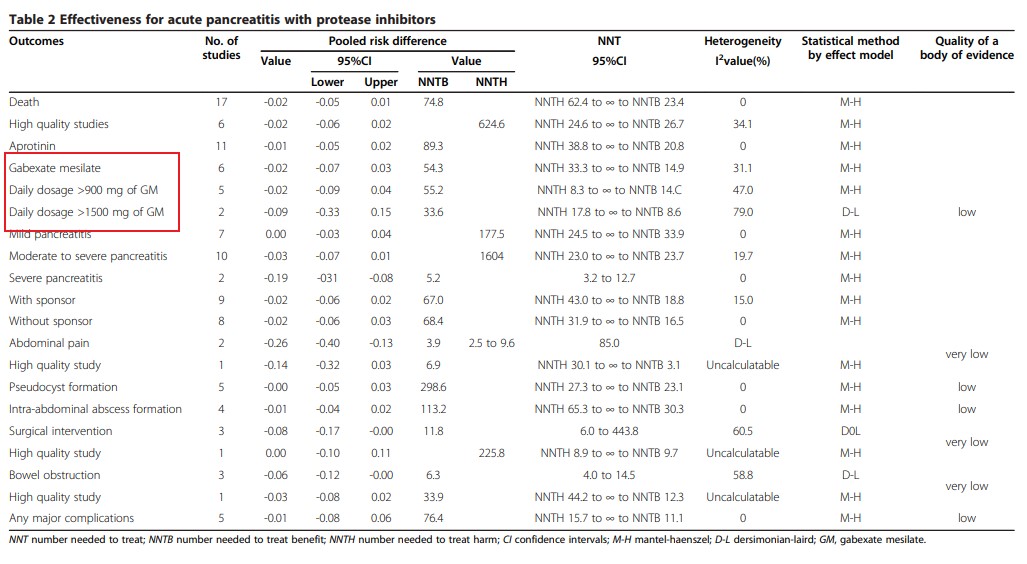
** gabexate(호의 주) 설명에서 다음 [4] 논문은 자세히 다루어 보겠다!
🙄 결론
: acute pacreatitis에 대한 nafamostat의 efficacy 자체는 controversial 하다. 고용량일 때에도 치료 성과에 대해서도 controversial 하다고 결론 내려야 되지 않을까 싶다. 하지만 prevention의 개념에서는 low risk patient에서는 high dose 사용 시 이점이 예상된다.
reference :
(1) Park, Kee Tae, et al. "Is high-dose nafamostat mesilate effective for the prevention of post-ERCP pancreatitis, especially in high-risk patients?." Pancreas 40.8 (2011): 1215-1219.
(2) 이준규, Recent Advances in Management of Acute Pancreatitis, Korean J Gastroenterol 2015;66:135-143
(3) Seta, Takeshi, et al. "Treatment of acute pancreatitis with protease inhibitors: a meta-analysis." European journal of gastroenterology & hepatology 16.12 (2004): 1287-1293.
(4) Seta, Takeshi, et al. "Treatment of acute pancreatitis with protease inhibitors administered through intravenous infusion: an updated systematic review and meta-analysis." BMC gastroenterology 14.1 (2014): 102.
'🤹♂️ 카테고리별 약물 > 위장관·췌장' 카테고리의 다른 글
| PPI 주사제 보험 심사 기준, 고시 제 2018-58호 (0) | 2020.08.19 |
|---|---|
| Stress ulcer prophylaxis, 스트레스 궤양 연관 위장관 출혈 예방, Famotidine, esomeprazole, pantoprazole (0) | 2020.08.19 |
| 기계 환기 받는 ICU 환자에게서 Stress ulcer prophylaxis with PPI vs. H2RA (0) | 2020.07.28 |
| domperidone(모티리움엠 정)과 metoclopramide(멕페란 정) 비교 (0) | 2020.07.22 |
| prucalopride 레졸로 정, 만성변비 (0) | 2020.06.21 |

댓글