
Pseudomonas aeruginosa 감염증의 외래 치료는 fluoroquinolones(FQ)에 대한 내성 증가율로 인해 어려움을 겪고 있다. 감수성 시험의 표준 방법에는 P. aeruginoosa의 azithromycin에 대한 활성을 나타내지 않는다. 그러나, azithromycin이 생체 내 환경을 재구성하는 생리학적 매체를 사용할 때 P. aeruginosa에 대해 매우 활성화되며 낭포성 섬유증(cystic fibrosis)을 포함한 다양한 임상 환경과 감염의 동물 모델에 근거들이 쌓이고 있다.
우리는 내성이나 환자의 intolerance으로 인해 FQ의 사용이 불가능했던 PO azithromycin으로 성공적으로 치료된 P. aeruginosa 이비인후과 감염의 세 가지 환자 관리 사례(Case report)를 제시한다. 우리는 이것이 임상의들에게 이 치료 옵션에 대해 경고하고 의학적 요구가 증가하는 환경에서 azithromycin에 대한 보다 철저한 임상 시험 평가에 영감을 줄 수 있기를 바라며 이 임상 접근 방식을 뒷받침하는 이전 데이터를 검토한다.
Historically, this drug has not been considered in the management of multidrug-resistant Gram-negative infections simply because it has no activity against these pathogens when tested in Mueller–Hinton broth—the gold standard media used for antimicrobial susceptibility testing in clinical laboratories across the globe.
Case 1
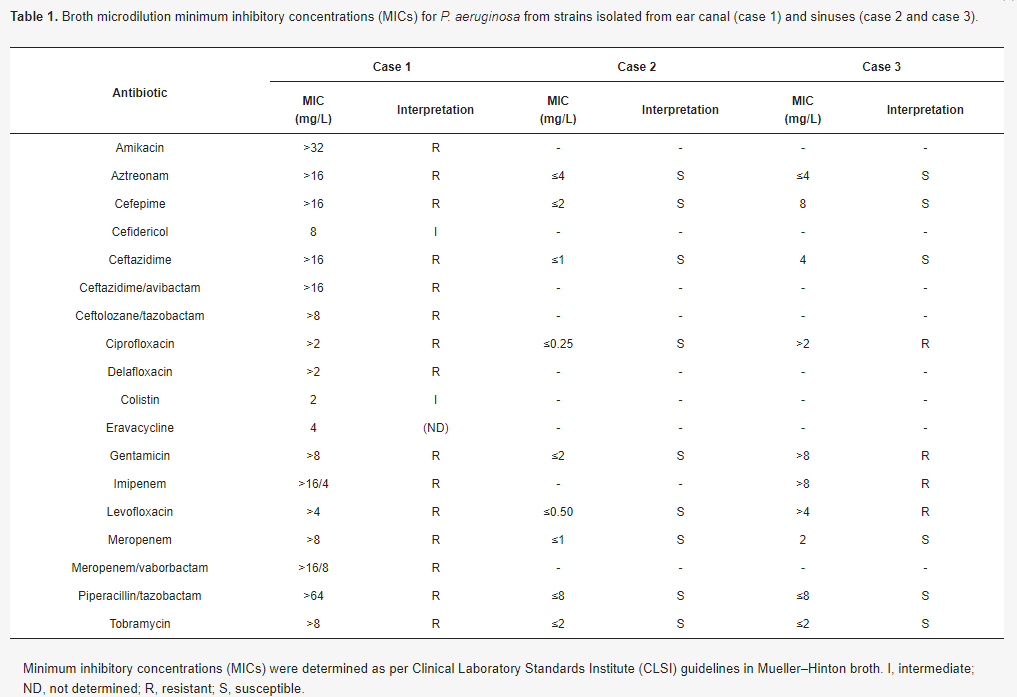
A male in his 60s developed bilateral ear pressure and drainage. Clinical history was pertinent for chronic ear pruritis and cerumen for which he used a metal pick to gently scratch his ear canals. There was no prior antibiotic history. The patient was evaluated by otolaryngology and underwent bilateral ear lavage. He was prescribed otic ofloxacin but developed a contact allergy and the drops were discontinued. Ear canal cultures were positive for methicillin-resistant Staphylococcus aureus (MRSA) and extensively drug-resistant (XDR) P. aeruginosa (Table 1). He denied having any fevers, chills, or headaches. He had had no international travel. He initially felt better, but symptoms recurred. Systemic antibiotics were prescribed (but never started), and he was referred to infectious diseases. Examination revealed an edematous right ear canal resulting in almost 50% occlusion with purulent drainage. The left ear canal had some purulent drainage but was not swollen. The patient was started on minocycline 100 mg PO every 12 h and azithromycin 500 mg PO every 24 h. Otolaryngology also compounded and prescribed a 2 to 3-week course of polymyxin ear drops. The ear purulence diminished somewhat but the right ear canal remained swollen. Oral antibiotics were continued. A CT scan showed no evidence of mastoiditis. Over the subsequent weeks the purulence resolved and the edema slowly improved. Total oral antibiotic therapy was continued for 8 weeks. He was strongly advised not to insert Q-tips or other objects in his ear canals. The patient showed no signs of relapse at 90 days after completion of therapy.
Case 2
A female in her 60s with diabetes mellitus, hypertension, and hypercholesterolemia was referred to infectious diseases for a 3-year history of recurrent sinusitis refractory to antibiotics. Symptoms would resolve with antibiotics but then recur. Within the past year, sinus cultures were positive for S. maltophilia, Staphylococcus epidermidis, and most recently, pan-susceptible P. aeruginosa. Symptoms included sinus pressure, congestion, and vertigo. No fevers, chills, or systemic symptoms other than fatigue due to lack of sleep from the above symptoms occurred. While the P. aeruginosa was susceptible to all reported antibiotics (Table 1), to minimize the risk of Clostridioides difficile, azithromycin 500 mg PO daily was prescribed. After 2 weeks, the vertigo resolved, and symptoms improved. Azithromycin was continued for 21 days with durable relief. Of note, due to the recurrent nature of the sinusitis, an immune workup was performed and revealed a lambda light chain in serum protein electrophoresis and the patient was referred to hematology.
Case 3
A female in her 60s was referred with a history of extranodal sinus lymphoma and recurrent sinusitis over several years secondary to methicillin-susceptible S. aureus (MSSA), MRSA, and P. aeruginosa. The most recent episode of sinusitis was due to P. aeruginosa, treated with levofloxacin. Symptoms of sinus pressure and pain returned, now yielding a quinolone-resistant P. aeruginosa (Table 1). The patient was subsequently treated with a 21-day course of azithromycin 500 mg PO daily with symptomatic improvement.

외이도염의 경우, XDR P. aeruginoosa 균주는 최신 항생제에도 적응할 수 없었다. 모든 경우에 치료는 매일 500mg의 아지트로마이신이었으며, 치료 기간은 P. aeruginoosa 단독 sinusitis 감염의 경우 3주, MRSA를 커버하기 위해 minocycline이 필요한 polymicrobial otitis externa의 경우 8주까지였다.
아지트로마이신은 수십 년 동안 이용 가능했던 잘 확립되고 안전한 항생제이다. 낭포성 섬유증 환자의 만성 관리에 있어서의 역할은 주로 항염증 효과이다. 이전 연구에서 보여주었듯이 항염증 효과는 직접적인 direct anti-pseudomonal activity 때문일 수 있다. 플루오로퀴놀론에 비해 아지트로마이신은 C. difficile 감염의 위험이 낮으며, 임신 및 소아과에서 더 확립된 이력이 있으며, risk of tendon and aortic rupture이 없다. 특히 항부정맥 약물을 복용하는 환자에서 QTC 연장의 위험이 있다는 것은 주목할 만한 사실이지만, 이는 우리 환자들에게는 문제가 되지 않았다.
우리는 P. aeruginosa의 대다수가 실제로 아지트로마이신에 감수성이 있다고 생각된다. 그러나 이러한 발견이 보편적인지 여부를 결정하고 시간이 지남에 따라 저항이 발생할 가능성을 평가하기 위해서는 더 큰 규모의 연구가 필요하다.
ref:
1) Ulloa, Erlinda R., and George Sakoulas. "Azithromycin: An underappreciated quinolone-sparing oral treatment for Pseudomonas aeruginosa infections." Antibiotics 11.4 (2022): 515.

댓글