Cortisol의 병태생리
- Stimulation of gluconeogenesis, catecholamine production, and activation of antistress and antiinflammatory pathways
- Essential for maintenance of cardiac output and contractility and enhancement of vascular tone via modulation of β-receptor synthesis and function and increased sensitivity to catecholamines, respectively
- 정상적인 부신은 5.7 mg(=15.7 μmol)/m²(체표면적)을 생성함. 이는 곧 180 cm의 75 kg 성인 남성이 하루에 약 30 μmol의 cortisol을 생성함을 의미(보통 8-10 mg/day cortisol을 생산)
- 내인성 cortisol을 생성할 수 없는 환자의 경우 외인성 보충량은 내인성 생산량의 2배 ⇨ 이는 biological availability & the first-pass metabolism of the liver를 극복하기 위함임
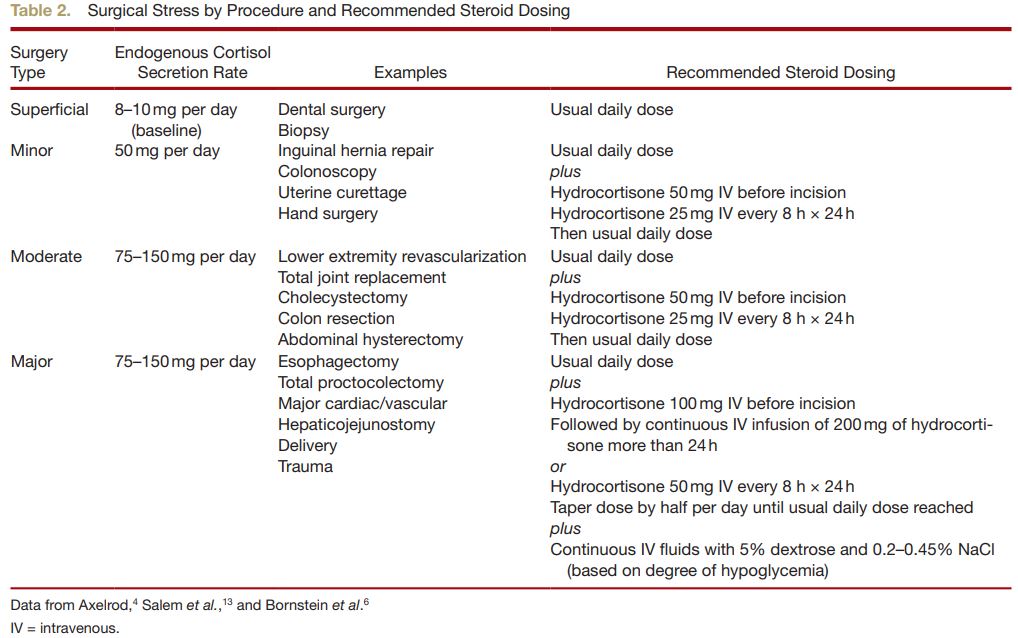
- 스트레스 상황(패혈증, 화상, 수술 등)에 대해 내인성 cortisol 생산은 5-6배 증가될 수 있음(200-300 mg) 혹은 경미한 시술의 경우 하루 최대 50 mg/day, 복잡한 시술의 경우 최대 75-150 mg/day이며 200 mg/day을 초과하는 경우는 드묾 [table2]
만성 스테로이드 치료로 인한 HPAA suppression 메커니즘

- HPAA(Hypothalamic-Pituitary-Adrenal Axis) suppression ⇨ low CRH and ACTH level ⇨ atrophy of the adrenal zona fasciculata and a decrease in cortisol production ⇨ secondary adrenal insufficiency, 특히 perioperative 기간 동안 adrenal crisis가 나타날 수 있음
- Primary adrenal insufficiency와의 차이점은 renin-angiotension-aldosterone system은 정상적으로 유지됨(no mineralocorticoid deficiency)
하지만 수술 중 마취 상태의 환자들에게서 일반적인 adrenal crisis 증상/징후(altered mental status, abdominal pain, nausea/vomiting, weakness, hypotension)를 관측하기 쉽지 않다. 임상적으로 "severe, persistent hypotension that is poorly responsive to fluid and vasopressor therapy" 발생 시 adrenal crisis를 의심해 볼 수 있다.
HPAA dysfunction을 유발하는 외인성 스테로이드의 용량 혹은 기간은 일반적으로 합의되지 않았지만 “prednisone 20 mg/day or its equivalent for more than 3 weeks”로 흔히 정의되고 있다. 하지만 실제 biochemical testing에 의하면 외인성 스테로이드 투여 용 & 투여 기간에 따른 HPAA 억제 수준과 치료 중단 후 정상으로 복구되는 기간은 잘 부합되지 않는다. HPAA 억제로부터 회복되는 시간은 개인마다 다르며 예측하기 어렵다. 그럼에도 불구하고 외인성 스테로이드 중단 1년 후에는 HPAA suppression이 지속되지 않을 것이라 동의한다.(with the possible exception of patients receiving intraarticular glucocorticoid injection)
Historical Perspectives
1949년, 코르티손은 primary adrenal insufficiency을 치료하기 위해 상업적으로 처음 생산되었고, 그 직후에 항염증 및 면역억제제로 사용되었다. 수술 중 스트레스성 스테로이드를 투여하는 역사적 근거는 1950년대 초반 두 가지 사례 보고서에 있으며, 각각 환자(n = 1)의 부검 결과를 근거로 cardiovascular collapse가 secondary adrenal crisis에 기인한다고 기술되었다. 그러나 두 사례 보고서 모두 교란 요인(confounding factor) 때문에 이후 비난을 받았다. 교란 요인에는 the withholding of aggressive fluid resuscitation, vasopressors, antibiotics, and most importantly the lack of biochemical proof of adrenal insufficiency via measurement of serum cortisol levels이 있다. 실제로 Brown and Buie은 adrenal crisis로 인한 수술시 저혈압은 드물며, 추정 발병률은 1~2%이며, 이 추정치는 1973년 Kehlet and Binder의 만성 스테로이드 치료를 받는 환자에게서 스테로이드가 중단된 환자 11명을 대상으로 한 prospective study에서 추정되었다. 그럼에도 불구하고 1950년대 초반 발생된 두 가지 사례 보고서를 근거로 HPAA 억제가 의심되는 환자에 대한 perioperative management가 요구된다.
만성 스테로이드 복용 중인 환자의 수술 시 드물지만 잠재적이면서 치명적인 합병증 예방을 위해 수술 중 stress-dose steroids 투여량을 고려해야 한다. 안타깝게도 여러 권고사항들은 일관성이 없다.
Unfortunately, this decision is not always clear-cut, because even the recommendations found in major textbooks are confusing, inconsistent, and lacking in class A and B evidence
다양한 reference에서의 perioperative Steroid 관리
① Miller’s anesthesia 8e
Acknowledge “a precise amount required has not been established”: IV 200mg/day hydrocortisone phosphate per 70kg of body weight or for minor procedure 100mg/day hydrocortisone phosphate per 70kg of body weight and then decreased at 25% per day until PO intake of maintenance dose can be resumed.
😁 70 kg 기준 200 mg/day hydrocortisone 혹은 minor procedure의 경우 70 kg 기준 100 mg/day → 하루마다 25%씩 감량하고 경구 투여가 가능할 때 재시작
② Clinical anesthesia 7e
Acknowledge both “an extensive review concluded that the best evidence was that patients should receive usual daily dose but no supplementation” and “many clinicians are unwilling to adopt the regimen until further trials have been undertaken in patients receiving physiologic steroid replacement” and ultimately give “popular regimen”: 200–300mg of hydrocortisone per 70kg of body weight in divided dose on the day of surgery, with adjustment in dose based on extent and duration of surgery and patients are to take their daily dose of steroids.
😁 70 kg 기준 200-300 mg hydrocortisone을 수술 당일 분복하여 투여한다. 수술 정도와 기간에 따라 용량조절이 필요하다.
③ Anesthesia and coexisting disease 6e
| Surgery | Recommendations |
| Superficial | Daily dose only |
| Minor | Daily dose plus hydrocortisone (25mg IV) |
| Moderate | Daily dose plus hydrocortisone (50–75mg, taper 1–2 days) |
| Major | Daily dose plus hydrocortisone (100–150mg, taper 1–2 days) |
④ UpToDate: The Surgical Patient Taking Glucocorticoids
Nonsuppressed (HPA) axis – defined as taking exogenous steroids for less than 3 weeks, or prednisone (<5mg daily or its equivalent) for any duration, or less than 10mg of prednisone or its equivalent every other day; we suggest continuing the same glucocorticoid regimen perioperatively (Grade 2C).
These patients are unlikely to have a suppressed HPA axis, and neither preoperative evaluation of the HPA axis nor supraphysiologic doses of glucocorticoids are needed.
😁 외인성 스테로이드를 3주 미만 혹은 prednisoloen으로 < 5 mg/day을 기간에 상관없이 복용한 경우를 nonsuppressed axis이며 이 경우, 수술 기간동안 같은 스테로이드 용량을 복용할 수 있다. nonsuppressed axis의 경우 HPA 축이 억제되지 않았을 가능성이 높으며 HPA 축에 대한 수술 전 평가나 supraphysiologic doses of glucocorticoids는 필요하지 않다.
In suppressed patients (defined as equivalent to prednisone 20 mg/day for 3 weeks or more), recommendations are surgery specific
😁 반면 prednisone으로 20 mg/day for 3wk 이상 투여받은 환자의 경우 수술 정도에 따라 다음과 같은 regimen이 권장될 수 있다.
| Surgery | Recommendations |
| Minor | Morning dose only |
| Moderate | Morning dose plus IV 50mg of hydrocortisone before incision; then IV 25mg every 8h for 24h and then maintenance |
| Major | Morning dose plus IV 100mg of hydrocortisone before induction; then IV 50mg every 8h for 24h; Taper dose by half per day to maintenance level |
⑤ Bornstein et al.: Diagnosis and treatment of primary adrenal insufficiency: An
Endocrine Society Clinical Practice Guideline
Acknowledge the “proposed glucocorticoid regimen in the management of adrenal crisis places a higher value on the prevention of underdosage than on reducing potential negative effects of short-term overdosage” as “under-dosing of glucocorticoids in an adrenal crisis is potentially hazardous. . . . Harm from these doses has not been shown, and direct studies indicating that lower doses are safe do not exist.”
Glucocorticoid dose adjustment based on severity of illness or magnitude of stressor, as follows:
| Surgery | Recommendations |
| Minor-moderate | Hydrocortisone, 25–75mg/24h (usually 1–2 days) |
| Major surgery, trauma, delivery, disease that requires intensive care, suspected adrenal crisis | Hydrocortisone 100mg IV followed by continuous IV infusion of hydrocortisone 200mg/24h (alternatively 50mg every 6 h IV/IM) |
The current and rather defensive strategy of perioperative supraphysiological glucocorticosteroid supplementation is not embedded in medical evidence. Additionally, high doses of glucocorticosteroids have disadvantages that should not be ignored. = 수술 중 초생리적 용량의 스테로이드가 필요한지에 대한 명확한 근거가 불확실할 뿐만 아니라 고용량의 스테로이드로 인한 부작용을 무시할 수 없음!
만성 스테로이드 사용 환자 관리에 대한 문헌과 논쟁이 증가하고 있다. 전반적으로 perioperative stress-dose steroid에 관해 A급 또는 B급 수준의 증거가 없으며 환자 개별화, 수술 및 마취 유형, 임상 결과, 스테로이드 기간 및 투여량 등 고려해야하는 요인이 많을 뿐만 아니라 일관성이 부족하므로 적정량 설정은 어렵다. perioperative stress-dose steroid에 대한 주제를 다루는 RCT는 매우 적을 뿐만 아니라 대상 환자수도 적고(대부분 20명 이하) insufficiently powered하다. 이는 통계적 분석을 거의 불가능하게 만드는 이유이다.
Current Evidence
| 1 | 아마도 perioperative stress-dose steroid에 대한 가장 강력한 데이터이다. - Methods 만성 스테로이드 치료(5 to 80 mg/day of prednisone or equivalent)를 받는 환자 73명을 대상 minor and major surgery 36시간 전부터 최소 24시간 이후 스테로이드를 중단 plasma cortisol level과 V/S를 모니터링 - Results 18명 중 7명이 설명되지 않는 저혈압 (defined as systolic blood pressure less than 80 mmHg not due to sepsis, anaphylaxis, or bleeding)을 경험 7명 중 3명이 low cortisol levels(defined in this study as less than 15 μg/100 mL)로 측정되었고 rescue steroid에 반응하지 않음 - Discussion 수술 전 혈장 cortisol 수치가 낮았던 환자들의 저혈압 가능성은 크게 높지 않았다. 저자들은 수술 전 혈장 cortisol 수치는 수술 중 혹은 수술 후의 만성 스테로이드 환자의 혈압을 결정하는 주요 요인이 아니며 스테로이드 치료를 중단하더라도 급성 스트레스로 인한 부신부전은 드물다고 결론 내렸다. 하지만 이에 합의된 정의(low cortisol level)는 없다는 점에 유의해야한다. 뿐만 아니라 이 연구에서 사용된 cortisol level 측정 방법은 오늘날 거의 사용되지 않는 fluorometric assay이며 이 때문에 applicability의 근거가 떨어진다. |
| 2 | - Methods cosyntropin study (also known as the short ACTH stimulation test)로 진단된 2차 부신부전으로 prednisone을 적어도 2개월 복용한 18명의 성인 남자 대상 various surgical procedures using different anesthetic techniques, including local, neuraxial, and general를 시행 수술 시행 전 stress-dose steroid 투여군(100 mg cortisol in N/S) vs 대조군(N/S) - Results hemodynamic parameter의 유의한 차이는 발견되지 않음 - Discussions 저자들은 2차 부신부전으로 만성 스테로이드 치료를 받는 환자에게 stress-dose steroid 투여가 없어도 저혈압을 겪지 않았고 usual daily dose of steroid를 perioperative period에 유지 가능하다고 결론 내렸다. 하지만 통계적인 차이(i.e., type II error)를 탐지할 수 있는 검정력이 충분하지 않다.(total n=18); insufficiently powered |
| 3 | retraction of a Cochrane review in 2013 “currently inadequate evidence to support the use of supplemental perioperative steroids in patients with adrenal insufficiency. It is likely that in the majority of adrenally suppressed patients undergoing surgery, administration of the patient’s daily maintenance dose of corticosteroid may be sufficient and that supplemental doses are not required.” Owing to the small number of patients, the results may not be representative. Based on current available evidence, we are unable to support or refute the use of supplemental perioperative steroids for patients with adrenal insufficiency during surgery. |
| 4 | Intraoperative hypotension that cannot be adequately managed by conservative means should raise suspicion for adrenal crisis, and a rescue dose of 100 mg of hydrocortisone IV should be administered, followed by continued supplementation of 50 mg of hydrocortisone IV every 6 h. |
| 5 | perioperative stress-dose steroid로 인한 위험성(immunosuppression, impaired wound healing, hyperglycemia, and psychologic disturbance)이 더 증가되었는지 여부는 무작위적으로 통제된 실험이 없기 때문에 논쟁의 여지가 있다. 후향적 renal transplant patients undergoing lymphocele surgery 환자를 대상으로 한 실험에서 저자들은 명백한 임상적 이점없이 고혈당 위험을 증가시켰다고 결론지었다. |
1. Kehlet H, Binder C: Adrenocortical function and clinical course during and after surgery in unsupplemented glucocorticoid-treated patients. Br J Anaesth 1973; 45:1043–8
2. Glowniak JV, Loriaux DL: A double-blind study of perioperative steroid requirements in secondary adrenal insufficiency. Surgery 1997; 121:123–9
3. Yong SL, Coulthard P, Wrzosek A: Supplemental perioperative steroids for surgical patients with adrenal insufficiency. Cochrane Database Syst Rev 2012; 12:CD005367
4. Bornstein SR, Allolio B, Arlt W, Barthel A, Don-Wauchope A, Hammer GD, Husebye ES, Merke DP, Murad MH, Stratakis CA, Torpy DJ: Diagnosis and treatment of primary adrenal insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2016; 101:364–89
5. Mathis AS, Shah NK, Mulgaonkar S: Stress dose steroids in renal transplant patients undergoing lymphocele surgery. Transplant Proc 2004; 36:3042–5
Our Approach
- Patients who have diagnosed secondary adrenal insufficiency as demonstrated by the short acting ACTH test. These patients will require perioperative stress-dose steroids with dosing based on surgical stress risk.
- Patients at high risk of HPAA suppression, including patients who have been treated with a glucocorticoid in doses equivalent to at least 20 mg/day of prednisone for more than 3 weeks or who have clinical features of Cushing syndrome. Unless data confirming the integrity of the HPAA is available, these patients would benefit from perioperative stress-dose steroids with dosing based on surgical stress.
- Patients at low risk of HPAA suppression, including patients who have been treated with any dose of glucocorticoid for less than 3 weeks, morning doses of prednisone 5 mg/day or less, or prednisone 10 mg/day every other day. Perioperative stress-dose steroids are not required unless they exhibit signs of HPAA suppression.
- Patients at intermediate risk of HPAA suppression, including any patient on chronic steroid therapy who does not fall into one of the above categories. If time permits, consider referring these patients for preoperative testing to determine their HPAA integrity. If testing is unavailable, the anesthesiologist must exercise his/her clinical judgment as to whether to administer stress-dose steroids based on the patient’s perioperative condition (e.g., degree of hemodynamic stability) and surgical risk. It is reasonable, for example, to withhold glucocorticoids if the patient is otherwise healthy and stable preoperatively without signs or symptoms of Cushing disease, with a low threshold for administration of a rescue dose of steroids in the event of unexplained intra- or postoperative hypotension.
| HPAA suppression | low risk | intermediate risk | high risk |
| 평소 스테로이드 복용량 | 용량과 상관없이 3주 미만 스테로이드 사용 혹은 morning doses of prednisone 5 mg/day or less |
중간 | 20 mg/day of prednisone for more than 3 week |
| 권장사항 | stress dose steroid 미권장 | 시간 여력이 된다면 test를 시행해보고 그렇지 못하다면 임상적 판단 | stress dose steroid |
2021.07.08: 오타 수정
Hydrocortisone
- Drug of choice for stress and rescue dose steroid coverage
- perioperative stress dose의 약제를 선택할 때, 2차성 부신부전의 문제는 glucocorticoid 결핍(not mineralocorticoid; 상대적 결핍)이라는 사실을 기억해야함!
- 따라서 약제별 glucocorticoid와 mineralocorticoid activity를 고려해야 함. mineralocorticoid activity 때문에 dose-dependent edema/fluid retention and hypokalemia가 발생할 수 있다.
- 예를 들어 hydrocortisone의 용량이 100 mg/day를 초과하는 경우, methylprednisolone으로 전환을 고려하는 것이 현명하다.

국내 glucocorticoid 경구제/주사제

추가 case (2021.07.08 추가)
원내 내분비내과에서 추천되는 stress steroid dosing resigmen
개인 병원에서 corticosteroid IV로 맞았던 투약력 있으며 지속적인 PO steroid 복용력은 확인되지 않는 환자
⇨ peak cortisol 수치 낮아 HPA suppression 가능성 있는 환자의 수술 전후 hormone replacement
- 수술 당일 : Hydrocortisone 100 mg IV → 50 mg q8h IV
- 수술 1일 째: Hydrocortisone 50 mg q8h IV
- 수술 2일 째: Hydrocortisone 50 mg q12h IV
- 수술 3일 째: Hydrocortisone 20-10 mg PO (8A, 4P)
- 수술 4일 째: Hydrocortisone 10-5 mg PO (8A, 4P)
reference:
1) Liu, Melanie M., et al. "Perioperative steroid management: approaches based on current evidence." Anesthesiology 127.1 (2017): 166-172.
2) de Lange, Dylan W., and Marleen Kars. "Perioperative glucocorticosteroid supplementation is not supported by evidence." European journal of internal medicine 19.6 (2008): 461-467.
3) Bornstein, Stefan R., et al. "Diagnosis and treatment of primary adrenal insufficiency: an endocrine society clinical practice guideline." The Journal of Clinical Endocrinology & Metabolism 101.2 (2016): 364-389.

댓글