
Normal saline(NS)는 일반적인 plasma와 비교했을 때에 비해 Cl-가 과량 함유되어있다.
전통적으로 알려진 NS의 문제점은 다음과 같다.
Metabolic acidosis & Hyperchloemia
| 신장 | Renal vasoconstriction: GFR decline Decrease in urine output Hypernatremia |
| 위장관 | Diminished visceral blood flow Disturbances of bowel motility |
| 기타 | Increase inlfammation Edema Inpaired wound healing |
🙄 Balanced crystalloid vs normal saline vs colloid 비교

1. New England Journal of Medicine 378.9 (2018): 829-839.
결론:
Among critically ill adults, the use of balanced crystalloids for intravenous fluid administration resulted in a lower rate of the composite outcome of death from any cause, new renal-replacement therapy, or persistent renal dysfunction than the use of saline.
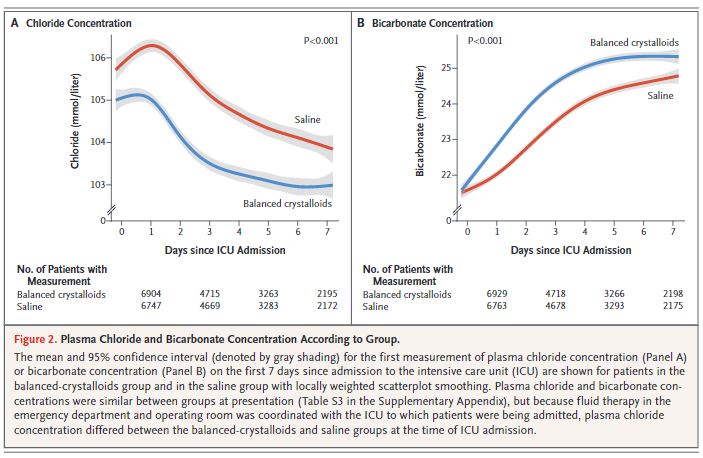
초기 balaned crystalloid에서 bicaronate가 잘 보존되기 때문에 이점이 있을 수 있다.(예상) 장기적으로는 유의한 차이는 없다.

내과 ICU, sepsis, TBI가 없는 환자군에서 balanced crystalloid가 더 favor 하다는 결과가 나왔다.
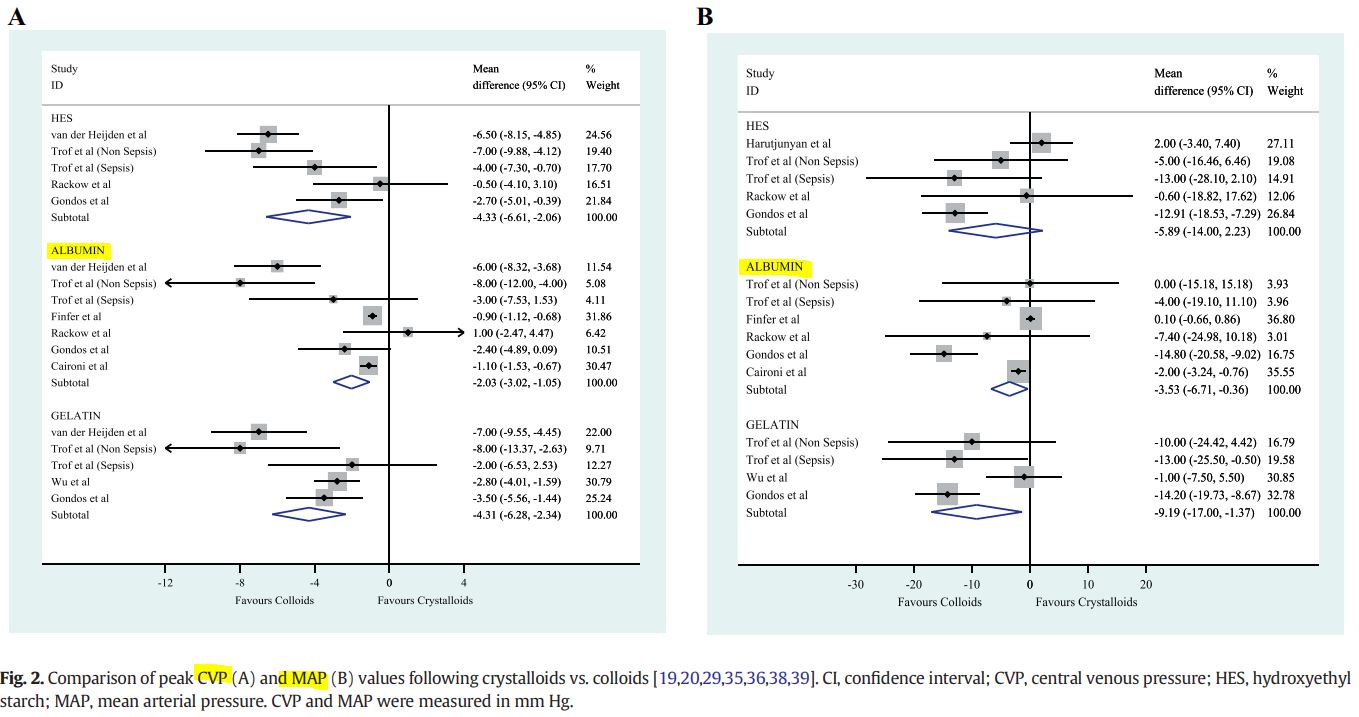
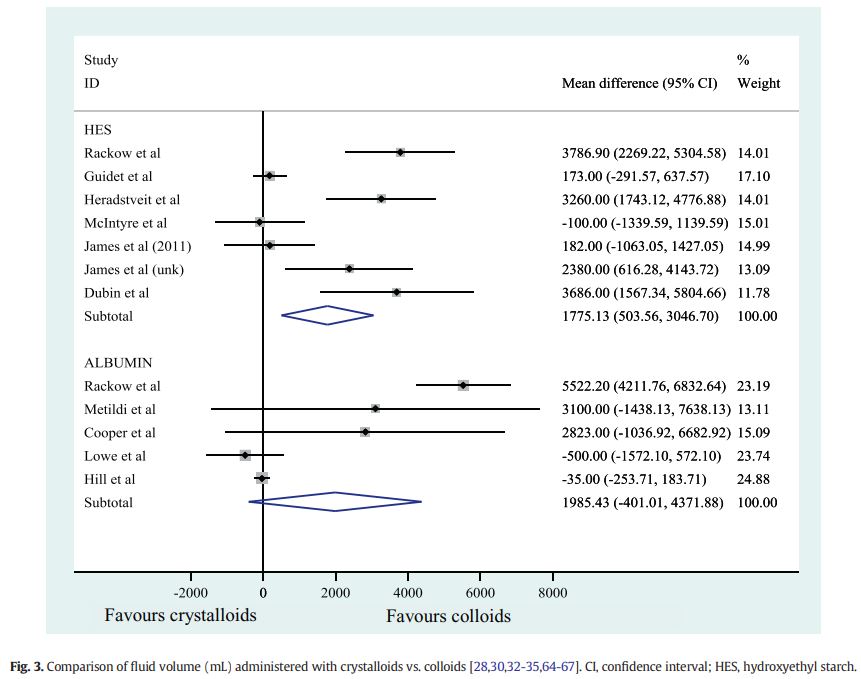
2. Journal of Critical Care 50 (2019): 144-154.
결론: 혈역학적 안정에는 crystalloid가 colloid에 비해 덜 효과적이다. ICU 상황에서 colloid보다 더 큰 volume을 필요로 한다.(이는 pulmonary edema 등의 유발하여 bad outcome이 나타날 수 있다.)
crystalloids were less effective than colloids at stabilizing hemodynamic resuscitation endpoints such as CVP, MAP, and cardiac index.
HES was the only colloid associated with increased mortality vs. crystalloids
Therefore, alternative fluid therapy with colloids such as albumin may be appropriate to restore hemodynamic endpoints in a more timely and effective manner.
- 알부민 급여기준
| 2016-08-01 | Albumin 주사제 | 고시 제2016-145호(약제) |
| ■ 고시 신설/개정 전체내용 1. 허가사항 범위 내에서 만성 저단백혈증으로 인한 급성 합병증을 치료 시 혈중 알부민 검사치가 3.0이하면서 아래와 같은 기준으로 투여하는 경우에 인정하며, 동 인정기준 이외 3.5미만의 저알부민혈증에 진료 시 필요하여 투여 시는 약값 전액을 환자가 부담토록 함. - 아 래- 가. 일반원칙 1) 저단백혈증으로 인한 Oncotic deficit(삼투압 결핍) 치료 2) 저단백혈증으로 인한 혈장 또는 혈량결핍 (Plasma or Volume deficit) 치료 나. 적응증 1) 쇼크(Shock) 2) 화상(Burns): 30%∼50% 이상 중증화상인 경우 24시간 이후 투여를 원칙으로 함. 단, 24시간 이전이더라도 crystalloids를 투여하였으나 반응이 없는 경우 인정 3) 성인호흡곤란증후군(Adult respiratory distress syndrome) 4) 심폐우회술(Cardiopulmonary bypass) 5) 신생아용혈병(Hemolytic disease of the newborn) 6) 급성 신증(Acute nephrosis) 가) 유효순환혈액량 부족 증상을 나타내는 경우 나) 고용량 이뇨제 투여에도 저항성을 보이는 급성 신증의 부종 치료에 이뇨제와 병용투여 시 단기간(7-10일) 인정 7) 아급성 또는 만성 저단백혈증(Subacute or chronic hypoproteinemia)(만성신질환, 만성간질환 등)로 인해 발생한 급성 합병증※의 치료 ※ 급성합병증의 예: ① 쇼크(Shock) ② 복수나 늑막삼출에 의한 호흡곤란(Dyspnea) ③ 부종(Edema) ④ 치료적 복수천자(대량의 복수천자로 인한 순환 불안정(Circulatory instability)이 있는 경우 등): 복수 3L~5L 천자 시 1병(20% 100mL), 5L 이상 천자 시 2병(20% 100mL) 인정 ⑤ 자발적 세균성 복막염(Spontaneous bacterial peritonitis): 진단 시 1.5g/kg, 3일째 1g/kg 투여 인정. 단, serum creatinine>1mg/dL 또는 BUN>30mg/dL 또는 total bilirubin>4mg/dL이어야 함 ⑥ 간신증후군(Hepatorenal syndrome): Type I에 혈관수축제와 병용 시 첫날 1g/kg, 이후 2~15일 동안 20~40g/day 인정 단, ④치료적 복수천자, ⑤자발적 세균성복막염, ⑥간신증후군은 혈중 알부민 수치에 관계없음 다. 금기사항(Contraindication) 1) 순환 혈장량의 증가에 따른 위험환자(예: 심부전, 폐부종, 핍뇨가 동반된 신부전 등) 2) 심한 빈혈(Severe anemia) 2. 허가사항 범위를 초과하여 아래와 같은 기준으로 투여 시 요양급여를 인정함. - 아 래 - 가. 뇌지주막하 출혈환자에게 볼륨확장(Volume expansion) 목적으로 5% 알부민주 투여 시 혈관조영(Angiogram)이나 도플러(Doppler), 자기공명영상진단(MRI) 등으로 Vasospasm(뇌혈관 연축)이 확인된 경우에 한해 혈중 알부민 수치에 관계없이 1-1.5g/kg/day 용량으로 7일까지 투여 시 요양급여를 인정하고, 그 이상 투여가 필요하여 투여한 경우에는 투여소견서를 첨부토록 함. 나. 개심술시 Osmorality(삼투압) 유지목적 또는 심근보호 목적으로 충전액이나 심정지액(Cardioplegic sol.)에 추가하는 경우 통상 1~2병(함량 관계없이 100㎖/1병 포장단위)을 인정함. 다. 혈장교환(Plasma exchange)시 사용한 알부민은 인정함[혈장분리교환술(Plasmapheresis)시 Eval Filter 사용하면 Albumin은 인정하지 아니함]. 라. 신이식술시 Plasmanate 대용으로 5% 알부민주 투여시는 알부민 수치와 관계없이 수술 당시에 2~3병정도 인정함. 마. 개심술 후 48시간 이내에 20% 100mL/1일 사용한 경우 바. 간이식 및 간절제 수술 후 혈중 알부민 검사치가 3.0 초과 3.5 이하인 다음과 같은 경우 3주까지 인정함 - 다 음 - 1) 중등도(grade 3) 이상의 요흔부종(pitting edema)이 있는 경우 또는 2) 1일 복수 배액량이 300mL 이상 나오는 경우 |
||
🙄 Resuscitation volume의 적정 용량, fluid의 PK data
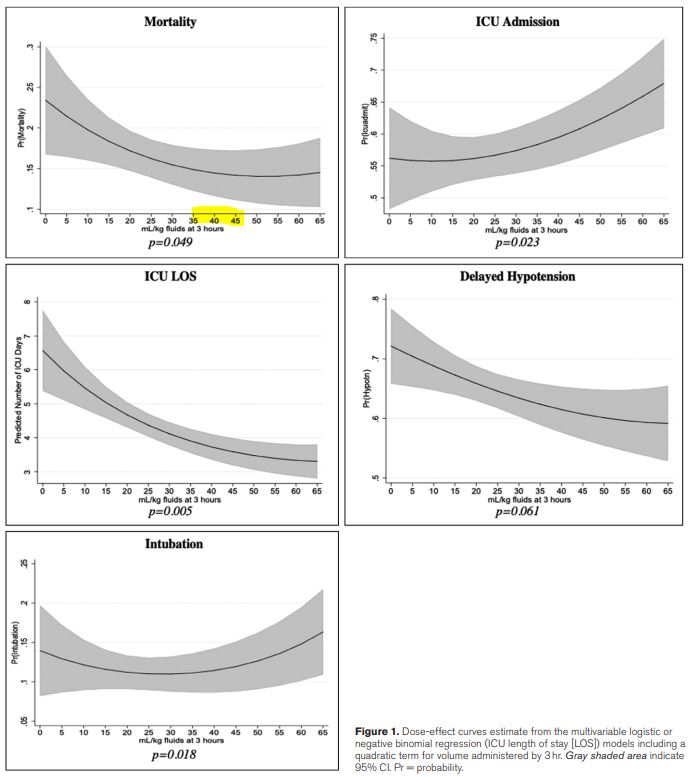
1. Critical care medicine 47.11 (2019): 1582.
* fluid 투여 속도 : If a start time to fluid resuscitation was documented without an end time, then fluids were assumed to infuse at 1 L/hr.
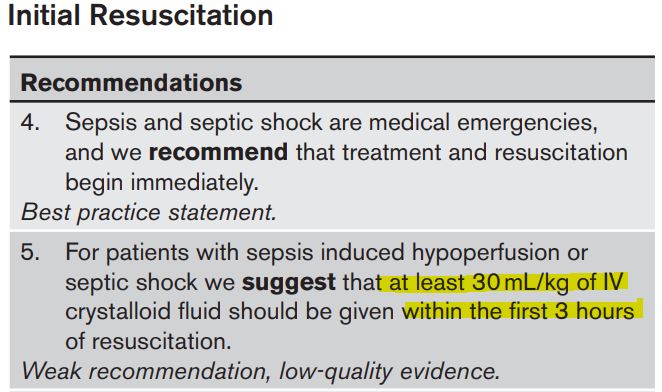
Finally, we attempted to examine what may be an optimal fluid volume. Our dose-effect curves suggest survival benefit with increased doses of fluids, plateauing between 35 and 45 mL/kg, supporting SSC recommendations. A more dramatic decrease in mortality is observed for patients receiving 0–10 mL/kg relative to the higher volumes, suggesting that a relationship between dosing of fluids, in addition to the timing, may influence odds of mortality. Interestingly, the same analysis also shows that the ~30–35 mL/kg volume to be the point at which the risk of intubation is the lowest, similar to a previous finding
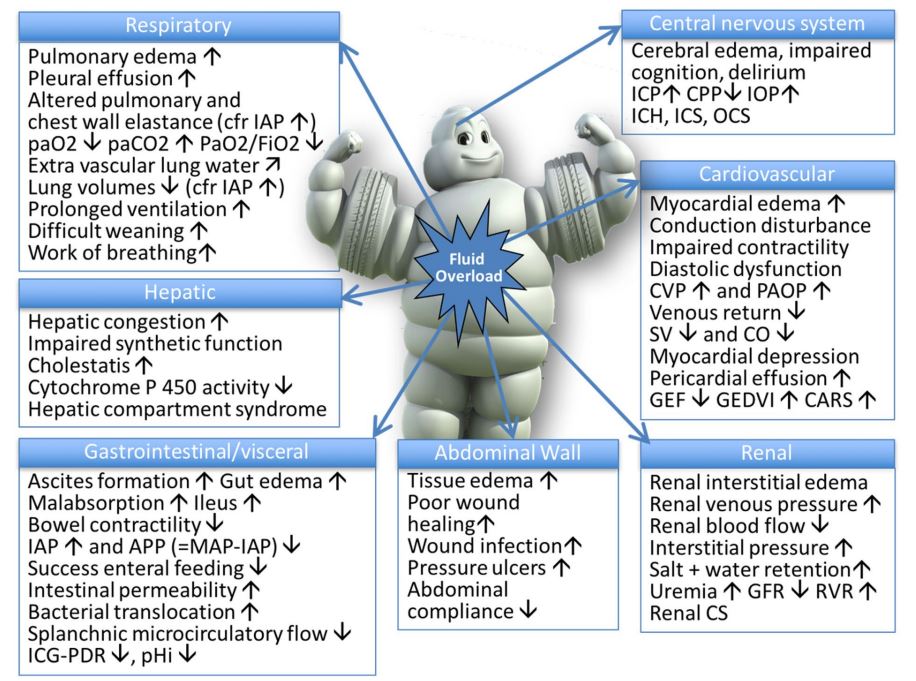
2. Annals of intensive care 8.1 (2018): 1-16.
Hypovolmeia is bad but hypervolemia is even worse.

Pharmacokinetics and pharmacodynamics fuids:
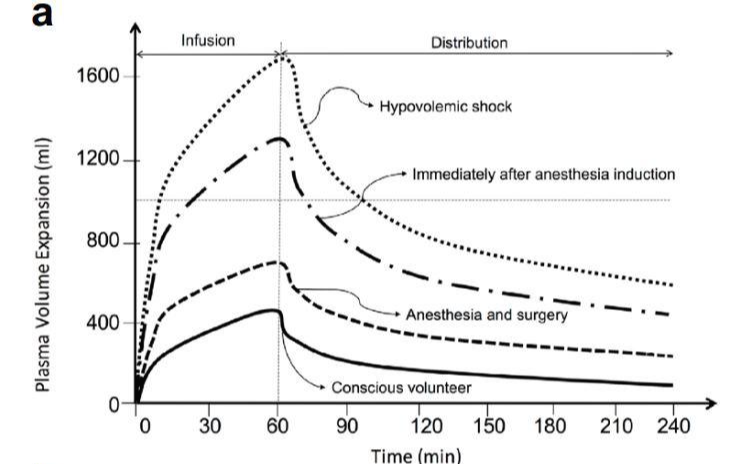
a Volume kinetic simulation. Expansion of plasma volume (in mL) after intravenous infusion of 2 L of Ringer’s acetate over 60 min in an adult patient (average weight 80 kg), depending on normal condition as conscious volunteer (solid line), during anaesthesia and surgery (dashed line), immediately after induction of anaesthesia due to vasoplegia and hypotension with decrease in arterial pressure to 85% of baseline, (mixed line) and after bleeding during haemorrhagic shock with mean arterial pressure below 50 mmHg (dotted line).
⇒ 환자 특성에 따라 다양한 volume expansion kinetic을 보인다.
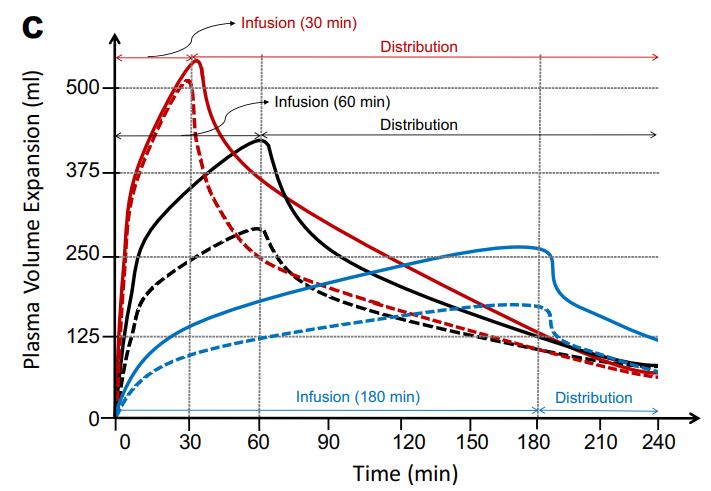
c Volume kinetic simulation. Expansion of plasma volume (in mL) after intravenous infusion of 500 mL of hydroxyethyl starch 130/0.4 (Volulyte, solid line) versus 1 L of Ringer’s acetate (dashed line) when administered in an adult patient (average weight 80 kg), over 30 min (red) versus 60 min (black), versus 180 min (blue). When administered rapidly and as long as infusion is ongoing, the volume expansion kinetics are similar between crystalloids and colloids, especially in case of shock, after induction and anaesthesia and during surgery.
⇒ fluid의 주입이 빠를수록 crystalloid와 colloid의 volume expansion kinetic은 유사한 경향성을 보인다.
reference:
1) Semler, Matthew W., et al. "Balanced crystalloids versus saline in critically ill adults." New England Journal of Medicine 378.9 (2018): 829-839.
2) Martin, Greg S., and Paul Bassett. "Crystalloids vs. colloids for fluid resuscitation in the Intensive Care Unit: A systematic review and meta-analysis." Journal of Critical Care 50 (2019): 144-154.
3) Evans, Laura, et al. "Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021." Intensive care medicine 47.11 (2021): 1181-1247.
4) Kuttab, Hani I., et al. "Evaluation and predictors of fluid resuscitation in patients with severe sepsis and septic shock." Critical care medicine 47.11 (2019): 1582.
5) Malbrain, Manu LNG, et al. "Principles of fluid management and stewardship in septic shock: it is time to consider the four D’s and the four phases of fluid therapy." Annals of intensive care 8.1 (2018): 1-16.

댓글