[2] Nutrition support in adult patients receiving extracorporeal membrane oxygenation
Timing of nutrition
초기 장내 영양은 안전성에 대한 우려가 있으며 특히 쇼크 상태로 인한 장기 관류의 감소와 고용량의 혈관 수축제의 사용은 더더욱 이러한 우려를 심화시킨다. 이러한 이유로 과거 ECMO 시, EN의 보류 혹은 최소한의 연기를 권장하였다. 하지만 최근 유럽 지침은 비록 전문가 의견에 근거하지만 조기 EN이 안전하고 실현 가능하다고 권고하였다.(safe and feasible)
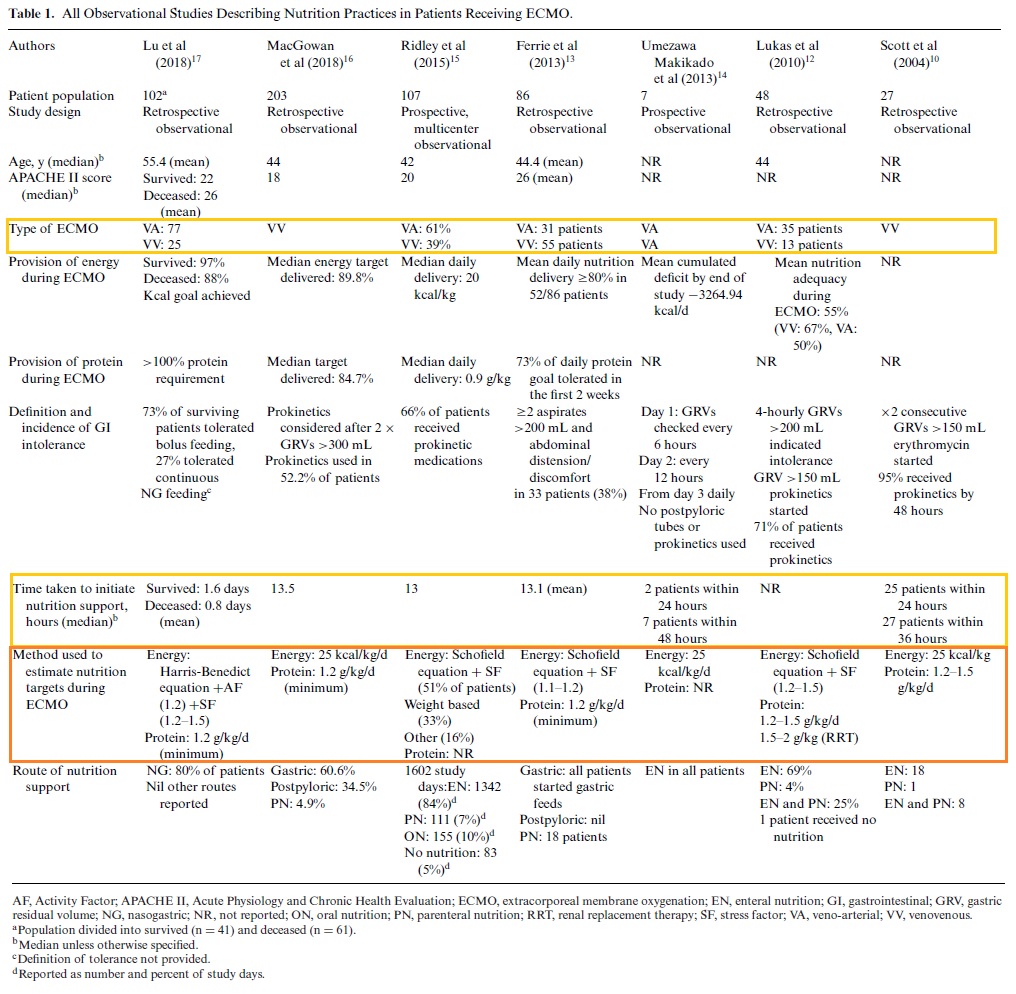
ECMO(VV/VA 모두 포함)를 받는 환자의 영양 관행(nutrition practice)에 대한 7개의 관찰 연구를 위의 표로 정리하였다. 이 연구에서 EN은 ECMO 시작 후 24시간 이내 시작하는 경우가 가장 많았으며 많은 연구에서 mean or median time=13hr로 보고되었다.
가장 N수가 많은 MacGrowan et al(2018)의 연구에 따르면 96%의 환자가 24시간 이내 EN을 시작하였다. feeding intolerance과 같은 부작용 보고는 드물지만, Ridley et al(2015) 연구에 의하면 107명 중 5명의 환자(4.5%)가 bowel ischemia가 나타났다. 해당 환자의 ECMO mode에 대한 데이터는 없었으며 부작용의 원인이 ECMO 때문인지 EN 때문인지 판단할 수 없다.
최근 쇼크로 인해 vasopressor support를 받는 환자에서의 EN vs early parenteral nutrition(PN)를 비교한 대규모 실험에서 28일 사망률에 큰 차이가 없었다. 하지만 EN군에서 위장관계 부작용 발생률이 더 높았다.
☝ severe shock 상태 환자에게 지원되는 VA ECMO의 경우, 고선량의 vasopressor의 사용 등으로 delay EN을 고려할 수도 있겠다.
Location of nutrition
대부분의 연구에서 영양 지원의 경로는 nasogastic feeding이다. postpyloric feeding은 드물게 나타나며 이는 튜브의 배치가 위 배치보다 어렵고 시간이 오래 걸리기 때문이다.
다른 나라에 비해 미국의 경우, ECMO 받는 환자에서 postpyloric feeding이 일반적으로 사용된다고 국제 조사에서 보고되었다.
PN의 사용 비율은 4-30%로 보고되었다. 정맥 지질이 ECMO의 lipid infiltration을 유발할 수 있다는 내용은 여전히 논란이 되고 있으나 이를 뒷받침하는 데이터는 제한적이며, 새로운 membrane은 이러한 위험이 적다. 따라서 현재로서 PN lipid 혹은 lipid가 함유된 약물을 투여해야 하는 ECMO 환자의 경우, membrane에 대한 면밀한 모니터링을 수행할 필요가 있다. transoxygenator gas exchange와 serum lipid의 모니터링 빈도는 1일 1회를 권장한다.
중성지방의 수치 > 300 mg/dL 시, lipid free PN tiwh weekly lipid + fat soluble vitamin 투여를 고려해야 한다.
Dose of nutrition support : 기본
중증 환자(critically ill)군의 에너지와 단백질 측면에서 최적의 영양 지원 선량에 대해 알려져 있지 않으며, 이는 ECMO를 받는 환자 역시 그러하다. ASPNE는 중증 환자에게서 nutrition risk scoring tool을 이용할 것을 권고하고 있으나, ECMO 환자의 경우, ECMO 시작 전 ICU 재원 기간으로 인해 실제 위험을 과소평가할 수 있기 때문에 이러한 환자들에게는 개인화된 영양 지원이 제공되어야 한다.
Dose of nutrition support : Energy
간접 열량 측정법(Indirect calorimetry)은 중증 성인의 energy expenditure(EE)를 결정하는 가장 first line choice이다.
간접 열량 측정법이란?
생체내에서 산소 소모량(VO₂)과 이산화탄소 생성량(VCO₂)을 측정하여 안정 시 에너지 소모량(resting energy espenditure)을 측정하는 검사법
판독 및 주의점
1) 산소를 사용 중인 환자에서는 산소 소모량이 흡입 산소량에 영향을 받기 때문에 정확한 값을 구하기 어려움
ex) FiO₂ > 60% 상황에서 정확한 값을 얻기 어려움
2) 이산화탄소 생성량은 호흡 형태에 따라 변할 수 있기 때문에 적어도 15-20분 동안 측정을 유지해야 함
한계
국내에서는 실제로 간접열량계를 사용 경험이 매우 적고, 기계의 조작이 어렵고 측정에 시간이 많이 걸리고 가격이 비싸다는 단점 등이 존재함. 보편화에 시간이 걸릴 것으로 생각됨
생체내에서 산소 소모량(VO₂)과 이산화탄소 생성량(VCO₂)을 측정하여 안정 시 에너지 소모량(resting energy espenditure)을 측정하는 검사법
판독 및 주의점
1) 산소를 사용 중인 환자에서는 산소 소모량이 흡입 산소량에 영향을 받기 때문에 정확한 값을 구하기 어려움
ex) FiO₂ > 60% 상황에서 정확한 값을 얻기 어려움
2) 이산화탄소 생성량은 호흡 형태에 따라 변할 수 있기 때문에 적어도 15-20분 동안 측정을 유지해야 함
한계
국내에서는 실제로 간접열량계를 사용 경험이 매우 적고, 기계의 조작이 어렵고 측정에 시간이 많이 걸리고 가격이 비싸다는 단점 등이 존재함. 보편화에 시간이 걸릴 것으로 생각됨

ECMO 중인 환자에게 IC를 이용하는 것은 native lung와 ECMO membrane을 통한 가스 교환, 재순환의 영향을 고려해야 한다. 재순환으로 인해 이산화탄소와 산소 교환 모두 과소평가될 수 있기 때문에 계산 시 오류의 원인이 될 수 있다.
IC를 사용할 수 없을 때, 일반적인 ICU 환자들에서 predictive or weight based equation을 통해 energy target을 설정하는 방법이며 이를 ECMO 환자에게도 적용할 수 있을 것이다.
measured energy expenditure(MEE)와 비교할 때, predictive based equation을 이용한 환자의 48%가 >500 kcal 더 과대평가되었다는 연구가 있다. 또한 weight based equation(25 kcal/kg)과 MEE 비교 시, EE를 상당히 과소평가하는 것으로 나타났다. 이러한 연구 결과는 6명의 환자를 대상으로 한 연구이긴 하지만 EMCO 중인 환자의 MEE가 평균 19 kcal/kg 밝힌 연구와는 상반된 결과를 보인다. 이러한 차이는 두 연구의 EE를 측정 방법이나 ECMO의 모드 차이 때문일 수 있다
아직까지 ECMO 환자에게 제공되는 영양지침이 없는 경우, 일반 중증 환자에 대한 지침을 따르는 것이 타당하다. (초기; 20-25 kcal/kg, recovery phase;25-30 kcal/kg from ESPEN)
ECMO 환자에서의 에너지 충족량에 따른 임상 효과; controversial, required to further findings
When considering the relationship of the dose of energy to clinical outcome in adult patients with ECMO, little data exist. However, receiving adequate energy intake (>80%) was associated with longer length of stay in 1 study.
It is not known whether this is simply due to the patients who remained in the ICU longer being able to reach nutrition targets, or whether there is a true burden associated with nutrition that increases length of stay.
→ 칼로리 충족에도 불구하고 재원기간이 길어졌다는 결과만으로 적절한 칼로리 충족이 임상 결과에 악영향을 끼쳤다고 해석하기보다는 다양한 상황 등을 고려하여 해석해야 한다.(ex 재원기간이 길어진 환자에서 점진적으로 증가되는 칼로리로 인해 다음과 같은 결과가 나왔을 수도 있음)
In contrast, in a retrospective study of Taiwanese patients receiving ECMO, achieving >80% of nutrition targets was associated with improved mortality. It is clear that prospective randomized controlled trials are required to further investigate these findings.
Dose of nutrition support : Protein
일반적인 중증 환자의 단백질 섭취에 대한 권장 사항은 1.2-2.5 g/kg/day이며 고선량의 단백질은 주로 비만, 화상, 외상 환자들에게서 적용될 수 있다. 이러한 권장 사항은 제한된 observational data를 기반으로 한다.
적절한 단백질 제공으로 인해 골격근의 감소를 예방할 수 있다.
ECMO를 받는 환자의 최적의 단백질 섭취량을 도출하기 위한 연구는 단 1개뿐이며, 본 연구는 적은 환자수로 VVECMO를 받는 비만/정상 환자의 질소균형을 조사하였다. 목표 단백은 정상 환자의 경우 1.5-2.0 g/kg/day, 비만 환자의 경우 2.0-2.5 g/kg/day였으며 목표 단백의 약 85%가 섭취되었다. 결과는 정상 환자에 비해 비만 환자에서 more negative nitrogen balance(−1.7 ± 5.7 vs −11.5 ± 9.6)를 보였다. 중증 환자에서의 질소 균형의 해석이 어렵다는 내재적 한계를 가지고 있음에도 불구하고 해당 결과는 환자들의 잠재적인 단백질 요구 사항에 대한 몇 가지 초기 통찰력을 제공하며 이 주제에 대한 추가적인 연구가 필요하다
negative nitrogen balance?
Negative nitrogen balance is associated with burns, serious tissue injuries, fevers, hyperthyroidism, wasting diseases, and during periods of fasting. This means that the amount of nitrogen excreted from the body is greater than the amount of nitrogen ingested.
ECMO 환자는 위의 권장 사항을 기반으로 최소 1.2 g/kg/day를 목표 단백 섭취량으로 한다. ECMO 환자에서의 단백질 섭취에 대한 현재의 권장 사항을 충족 시, 근육 소실 완화 등의 임상 결과가 개선되었는지에 대해서는 알 수 없다.
Barriers to the delivery of EN
delayed gastric emptying은 ECMO 환자에서 EN 관련 합병증 중 하나이다. 하지만 delayed gastric emptying의 정의는 위잔류량(GRV)에 근거하며, 150-300 mL의 다양한 임계값이 존재한다.
Bedside and operating room procedures는 EN의 중단의 대부분의 이유이며 volume based feeding 방식을 통해 poor delivery of nutrition을 예방할 수 있을 것이다. 하지만 ECMO 환자에서의 volume based feeding에 대한 연구는 아직까지 진행될 것이 없지만 더 안정한 상태의 환자에게서 옵션으로서 제외할 필요는 없을 것으로 생각된다. 추가적인 명백한 근거가 나오기 전까지 일반 중증 환자의 권장 사항을 외삽하여 사용하여도 무방하다고 생각된다.
volume based feeding?
“volume-based” goal represents a significant shift in practice from traditional hourly rate goals in which nurses can increase the hourly rate depending on how many hours they have left in the day to ensure that the patient receives the 24-hour volume within the day.
Studies planned or in progress
- Measuring Energy Expenditure in ECMO (Extracorporeal Membrane Oxygenation) Patients (MEEP) (NCT01992237) aims to describe a calculation to determine nutrition targets in patients receiving ECMO. Secondary aims include describing levels of nutrition needs for different mechanical ventilation states, and to use oxygen and carbon dioxide elimination to estimate cardiac output.
- The use of Computed Tomography (CT) to Measure Skeletal Muscle Quantity and Quality in Patients Receiving ECMO (NCT03269825) aims to investigate the clinical predictive value of and change in muscle quantity and quality in patients receiving VV ECMO. Secondary aims are to determine any relationship between total nutrition received and change in muscle quantity and quality.
- Characterizing changes in muscle quantity and quality in patients requiring ECMO during critical illness (ECMO USS) (NCT02995811) aims to identify changes in different muscle groups (trunk, respiratory, and skeletal muscle) in patients receiving ECMO. The association between nutrition and changes in muscle quality and quantity will also be addressed.
- Progressive Rehabilitation Therapy in Patients with Advanced Lung Disease (NCT 03562728) aims to investigate the impact of a multimodal rehabilitation program in ameliorating the loss of muscle mass and strength, and lower extremity balance, strength, and coordination in patients requiring lung transplant or ECMO as a bridge to transplant. The multimodal rehabilitation program includes neuromuscular electric stimulation, strength and mobility training, and nutrition supplementation with amino acids 3 times daily.
Potential research questions
- What is the optimum energy intake in patients receiving VV and VA ECMO?
- What is the optimum protein intake in patients receiving VV and VA ECMO
- What is the impact of nutrition support on the physical and functional recovery of patients receiving VA and VV ECMO?
- What are the optimum energy and protein targets during rehabilitation in patients receiving ECMO?
- Are nutrient losses (micronutrients and macronutrients) present across the ECMO membrane, and are these losses clinically meaningful?
reference:
1) Thibault, Ronan, et al. "Nutrition of the COVID-19 patient in the intensive care unit (ICU): a practical guidance." Critical Care 24.1 (2020): 1-8.
2) Bear, Danielle E., Elizabeth Smith, and Nicholas A. Barrett. "Nutrition support in adult patients receiving extracorporeal membrane oxygenation." Nutrition in Clinical Practice 33.6 (2018): 738-746.
3) Lee, Kwan-Ho. "호흡기 질환에서의 간접 칼로리 측정과 응용."
4) 대한 외과 대사 영양학회 뉴스레터, 2018 제7호 [영양 관련 최신지견] 중환자 영역에서의 영양; 이재명
5) wikipedia
'👩⚕️Px 영역 > TPN·영양' 카테고리의 다른 글
| Vitamin K 투여 경로, IV vs IM vs SC (0) | 2021.03.25 |
|---|---|
| 경장영양, enteral nutrition(EN): trophic feeding, full feeding (0) | 2021.03.14 |
| ECMO 환자, 영양, nutrition, TPN_1편 (0) | 2021.03.12 |
| 경장영양 모니터링: 위액 배액/ 배관, gastric residual volume(GRV) (0) | 2021.03.03 |
| 가이드라인 별 lipid 권고 사항(ASPEN, ESPEN, Canadian) (0) | 2020.12.20 |

댓글