Optimal norepinephrine-equivalent dose to initiate epinephrine in patients with septic shock
- Norepinephrine-equivalent dose at epinephrine initiation that correlated with hemodynamic stability was evaluated.
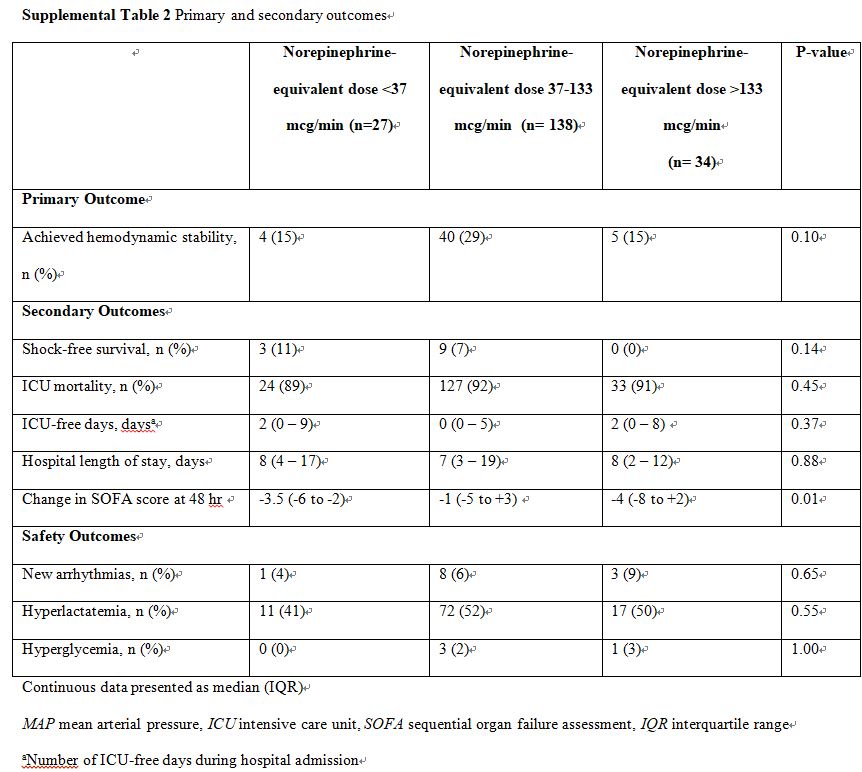
- Initiation of epinephrine at norepinephrine-equivalent doses of 37–133 μg/min was associated with hemodynamic stability.
- No differences were observed in shock-free survival, change in SOFA, ICU-free days, lactic acidosis, and new-onset arrhythmias.
- The incidence of hemodynamic stability after epinephrine initiation was low.
| 목적 | 패혈증 쇼크 시, epinephrine(EP) 투여가 필요한 시점의 norepinephrine(NE)의 명확한 용량이 명확하지 않음 이번 연구를 통해 혈류역학적 안정성과 상관관계가 있는 EP 시작 시 NE-equivalent dose를 결정하기 위해 노력함 |
| 방법 | NE와 EP가 투여된 패혈증 쇼크 환자를 포함 Classification and regression tree analysis을 이용하여 NE-equivalent dose의 breakpoint를 결정 primary outcome : 혈역학적 안정성(hemodynamic stability) secondary outcome : shock-free survival, time to achieve hemodynamic stability, change in SOFA score. |
| 결과 | norepinephrine-equivalent dose : 37 - 133 μg/min ⇒ (약 0.6-2.2 mcg/kg/min(ɤ) ; 60 kg 기준) optimal dose group : 138명 non-optimal dose group : 61명 optimal dose group에서 혈역학적 안정성 도달 비율이 더 높음 최적 NE equivalent dose range 내에서 EP 투여를 시작하는 다변량 분석에서 혈류역학 반응의 높은 odds과 독립적으로 연관되었음(OR 3.06 [95% CI 1.2-7.6]; p=0.02) |
| 결론 | 적절한 NE dose 범위(37-133 mcg/min)로 투여 중, EP 투여를 시작하는 경우 혈역학적 안정성과 더 높은 연관성이 있음 |
2016 Surviving Sepsis Campaign guideline에서 적절한 fluid bolus 처치에도 MAP(mean arterial pressure) 유지가 되지 않는 환자에게서 6시간 이내 vasopressor을 투여할 것을 권고하고 있음
그중 NE는 1st line이며, EP의 경우 2nd line임
하지만 NE에 반응이 부족한 환자에게서 어떻게 얼마나 다른 vasopressor을 투여할지에 대한 데이터는 부족한 실정임
이러한 이유로 2차 약제의 개시는 주로 임상의 선호나 제한된 증거에 근거한 프로토콜에 의해 추진되었음
NE는 주로 systemic vascular resistance ↑ vs. EP는 both systemic vascular resistance and cardiac output ↑
패혈증 쇼크일 때 적절한 fluid resuscitation으로 cardiac output이 증가하기 때문에 EP 추가에 의한 inotropy 효과의 이점이 불분명함
문헌적으로 다양한 NE equivalent dose range가 존재함, 뿐만 아니라 practice decision을 더 복잡하게 하는 것은 EP 투여를 지지하는 가이드라인은 EP의 역할이 2차 선택약이 아닌 1차 선택약이라는 점임
2차 vasopressor 개시 시점에 대한 전반적인 데이터가 부족하기 때문에 이상적인 vasopressor 사용에 대한 더 나은 이해가 필요. 이러한 이유로 본 연구에서 패혈성 쇼크 환자에 대한 최적의 EP 시작을 위한 NE equivalent dose range를 정의하고자 함
METHODS
non-interventional, retrospective cohort study
18세 이상의 medical/surgical/neuroscience ICU 환자 중 septic shock으로 일차 vasopressor로 NE를 적어도 1시간 이상 투여받은 환자
septic shock 정의 : SOFA score 2점 이상 & lactate 2 mmol/L 이상
primary outcome : EP 투여 이후, 혈역학적 안정성 도달
* 혈역학적 안정성 : 2회 연속 down-titration in vasopressor dosage requirement & 이후 8시간 동안 추가적인 용량 증량 없이
모든 vasopressor requirement는 NE equivalent dose에 기반하여 평가됨
혈역학적 데이터와 vasopressor requirement는 NE와 EP 투여 24, 48, 72 hr 이후, EP 투여 7 day 이후에 각각 측정됨
secondary outcome : 혈역학적 안정성 도달 시간, shock free survival, EP 투여 48시간 뒤 SOFA 점수 변화, ICU free day, 재원일수
* 혈역학적 안정성 도달 시간 : EP 투여 이후부터 첫 down titration 한 시간(end point 만족한 시기 동안)
* shock free survival : EP 투여 7일 이후 생존 & 모든 vasopressor 중단 시
* SOFA 점수 변화 : EP 개시 후 48시간 이내 생존한 환자의 SOFA 점수
safety outcome : EP 투여 첫 8시간 동안 발생한 hyperglycemia, hyperlactatemia, new onset arrhythmias
* hyperglycemia : 혈당 180 mg/dL 이상 or insulin 투여 시작
* hyperlactatemia : baseline에 비해 1 mmol/L 이상 상승 시
* new onset arrhythmias : 심박수 >140 beats/min시 혹은 심박수 악화
RESULT
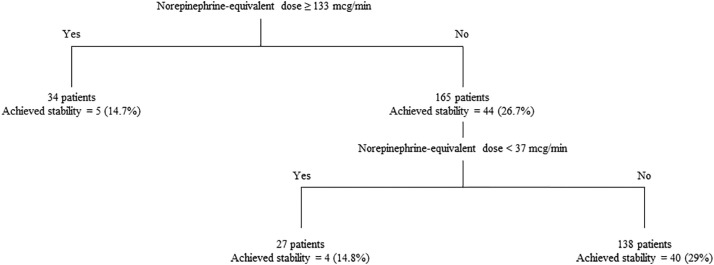
The CART analysis identified two significant breakpoints in norepinephrine-equivalent dose at epinephrine initiation associated with hemodynamic stability.
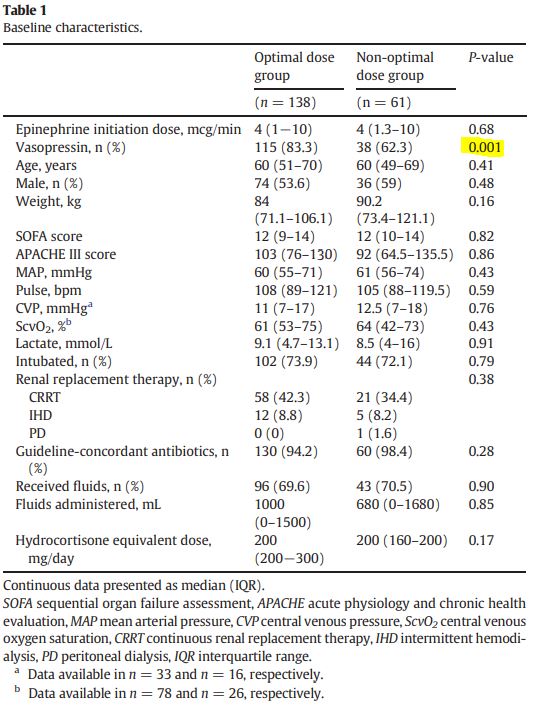
vasopressin 사용은 optimal dose group에서 유의하게 더 많음(115 [83.3%] vs. 38 [62.3%]; p =. 001) 그 외 인구통계학적 특성은 두 군에서 비슷함
In the Cox proportional hazards model, receiving norepinephrine-equivalent doses between 37 and 133 μg/min at epinephrine initiation was associated with an increased rate of achieving hemodynamic stability (HR 2.09 [95% CI 1.01–4.30]; p = .05)
After adjustment for vasopressin use, SOFA, MAP, and lactate with multivariable logistic regression, initiating epinephrine within the optimal norepinephrine-equivalent dose range was independently associated with higher odds of hemodynamic response (OR 3.06 [95% CI 1.2–7.6]; p = .02)
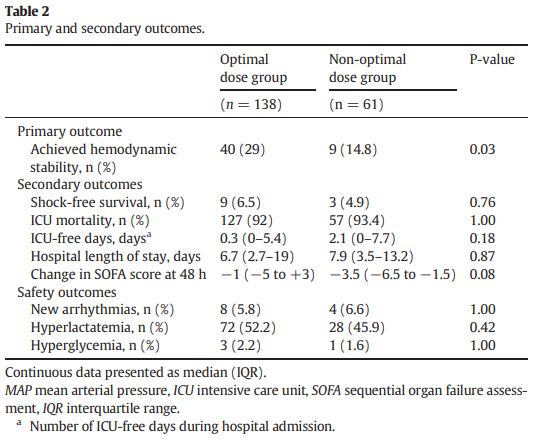
primary outcome을 제외한 다른 outcome에는 유의한 차이가 없음
DISCUSSION
(아마) adjuctive EP 개시를 위한 최적의 NE 용량을 평가하는 첫 번째 연구임
CART 분석을 이용하여 이 모집단에서 역 U자 모양으로 혈류역학적 안정성에 해당하는 두 개의 투여 중단점을 확인할 수 있었음
NE 투여량 중단점 전 후의 용량을 투여받은 환자는 생리학적 상태가 다를 수 있지만, 결론적으로 EP가 너무 빨리 시작되거나 너무 늦게 시작되면 더 나쁜 결과를 얻을 수 있음
이는 기존에 선형 dose-response 관계를 평가하는 기존의 약리학적 연구와는 다름
| <37μg/min | 37–133 μg/min | > 133 μg/min |
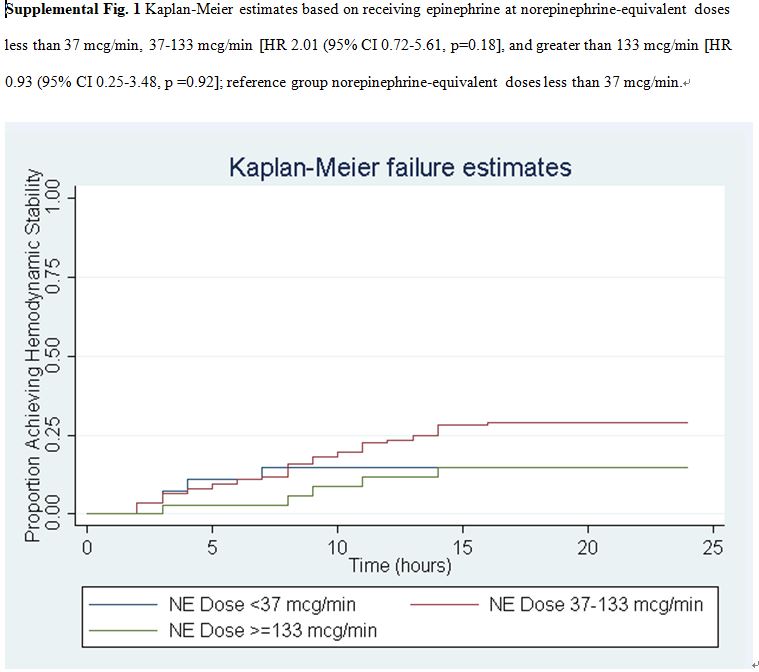
각 군에서의 예후의 차이는 없었음(supplemental data 참조)
각 군에서 hyperlactatemia 부작용이 흔함. 특히 EP 투여 군에서 lactate 증가가 흔히 보고되는데, 이는 약제로 인해 혐기성 당분해(aerobic glycolysis)가 증가되기 때문. 따라서 EP associated hyperlactatemia는 acidemia를 유발하고 임상의로 하여금 tissue perfusion 악화와 약제 유발 ADR과의 구별에 혼돈을 야기하여 약제의 임상적 효용성이 제한될 수 있음
However, in this study it did not translate into meaningful clinical outcomes. We hypothesize that perhaps these positive clinical outcomes were not identified due to lack of statistical power to detect these outcomes. As such, adequately powered studies should further investigate the clinical significance of these norepinephrine-quivalent dose breakpoints.
In conclusion, epinephrine initiation at a norepinephrine-equivalent dose between 37 and 133 μg/min correlated with hemodynamic stability in this study of septic shock. Thus, clinicians should consider the addition of epinephrine when doses of other vasopressors have been optimized and should not significantly delay initiation of epinephrine until the norepinephrine-equivalent dose is >133 μg/min. Norepinephrine-equivalent dose is one of many patient-specific factors that clinicians should consider when adding epinephrine in patients with septic shock.
reference :
(1) Ammar, Mahmoud A., et al. "Optimal norepinephrine-equivalent dose to initiate epinephrine in patients with septic shock." Journal of critical care 53 (2019): 69-74.
'🤹♂️ 카테고리별 약물 > 심혈관' 카테고리의 다른 글
| beta blocker, adverse drug effect, ADR, hypoglycemia, hyperglycemia (0) | 2020.11.20 |
|---|---|
| Beta blocker(베타차단제), class effect, 심장선택성 (0) | 2020.11.19 |
| Effect of norepinephrine dosage on mortality in patients with septic shock (0) | 2020.11.15 |
| COPD 환자에서의 베타차단제, beta blocker와 lung function (0) | 2020.10.26 |
| 비만 환자(obese), 크렉산 주(enoxaparin)의 VTE 예방(prophylaxis) & 치료(treatment) (0) | 2020.10.13 |

댓글