1. In adult critically ill patients, does provision of higher vs lower energy intake impact clinical outcomes?
- No significant difference in clinical outcomes was found between patients with higher vs lower levels of energy intake. We suggest feeding between 12 and 25 kcal/kg (ie, the range of mean energy intakes examined) in the first 7–10 days of ICU stay.
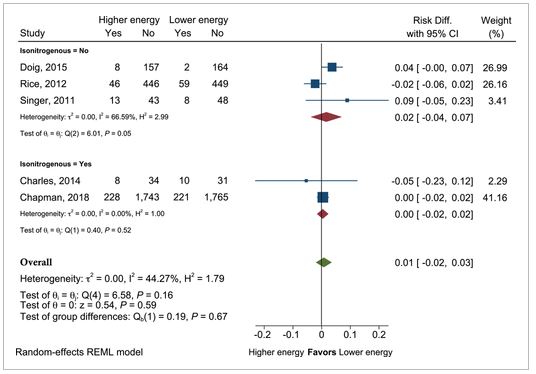
Mean difference in bacteremia in patients with higher vs lower energy intake
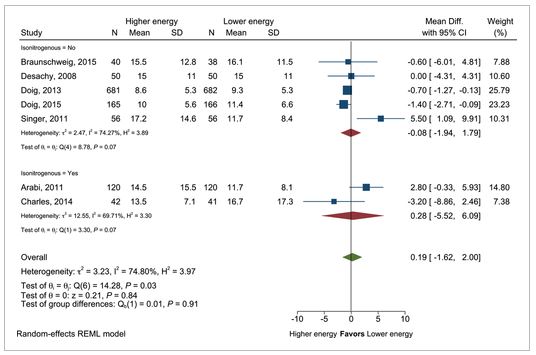
Mean difference in intensive care unit length of stay in patients with higher vs lower energy intake
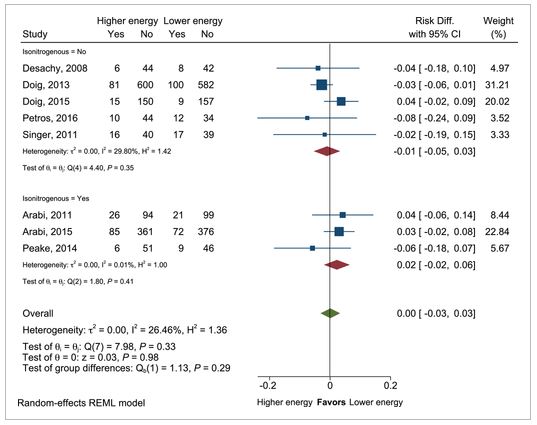
Mean difference in intensive care unit mortality in patients with higher vs lower energy intake
이번 가이드라인(2021)은 nutrition risk or ARDS을 기반으로 다양한 지침을 제공했던 이전 버전과 다르다.
2016년 가이드라인에서는 영양 위험(nutrition risk)을 평가하여 (1) low nutrition risk 환자에서는 전문 영양 요법(specialized nutrition therapy)을 권장하지 않았으며 (2) ARDS 환자에서 trophic or full dose EN을 권고하였다. 또한 (3) high nutrition risk 환자에서는 48-72시간 이내 에너지 요구량의 80% 이상을 달성할 것을 권장하였다.
이러한 권고는 영양 위험도 점수에 따라 환자의 영양 필요 정도가 달라질 것이라는 이론에 근거하였다. 이것은 RCT 데이터 등으로 뒷받침 or 반박되지 않았다.
에너지 섭취와 관련하여 통계적으로 또는 임상적으로 유의미한 결과 차이를 발견하지 못했다는 사실을 고려하여 이번 지침에서는 영양 위험 구별(distinction of nutrition risk)을 유지하지 않기로 결정하였다.
실제 가이드라인에 수록되어있는 수많은 연구에도 불구하고 higher or lower energy에 대한 정의 방법의 불일치로 의미 있는 결과를 이끌어 내기 어려웠다.
문헌들의 이질성이 높을수록 중증 환자에서 섭취량의 많고 적고의 따른 평균적인 상대적 효과 외에는 추론할 수 없다.
중증 환자의 초기 영양 섭취 보류(withholding feeding)에 대한 RCT 데이터가 부족하기 때문에 해당 근거는 권장 사항에서 제외되었다.
partial PN(supplement parenteral nutrition; SPN) or PN은 EN의 불내성인 환자에서 고려될 수 있다.
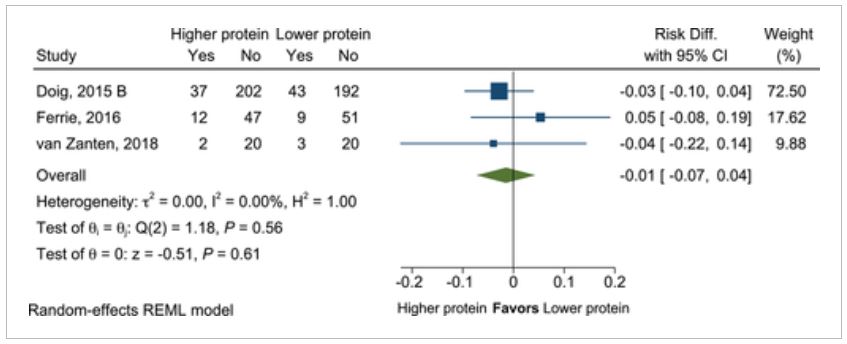
2. In adult critically ill patients, does provision of higher as compared with lower protein intake impact clinical outcomes?
- There was no difference in clinical outcomes in the relatively limited data. Because of a paucity of trials with high-quality evidence, we cannot make a new recommendation at this time beyond the 2016 guideline suggestion for 1.2–2.0 g/kg/day.
단백질 함량에 따른 임상 결과를 분석하기 위하여 (1) 단백질 섭취량을 g/kg/day로 보고 (2) 그룹 간 단백질 섭취량의 차이가 최소 0.2 g/kg/day 이상 (3) 그룹 간 칼로리 섭취량이 대략 동등한 연구를 추려 총 4개의 임상, 697명의 환자가 이러한 기준을 충족하였다.
고단백 군으로 추출된 군에서의 단백 섭취량은 1.119-1.3 g/kg/day이다. 각 연구 결과들은 상이하고 증거의 질이 다르며 표본의 크기가 작은 연구도 있기 때문에 제한된 데이터에 기초하여 권고안이 만들어졌다.
Mean difference in intensive care unit mortality in patients with higher vs lower protein dose.
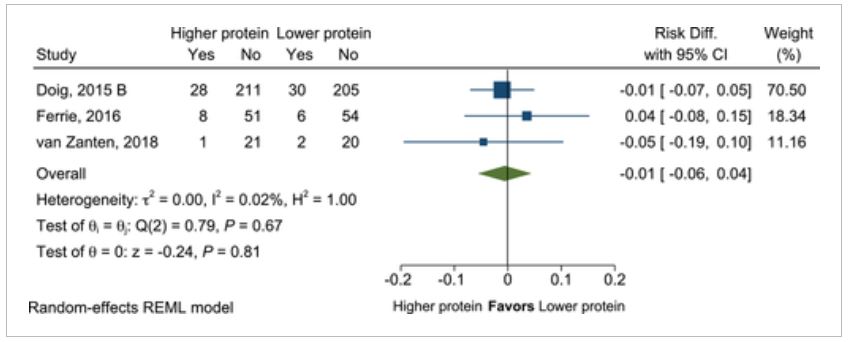
Mean difference in hospital mortality in patients with higher vs lower protein dose.
2016 발표된 ASPEN-SCCM 가이드라인에서는 중증 환자, 화상, 비만, 외상 환자에게 더 많은 양의 단백질을 제공할 것을 권장하였다. 현재 가이드라인에서도 이용 가능한 단백질 섭취 양의 영향에 대한 RCT는 제한적이다. 또한 해당 군(중증 환자, 화상, 비만, 외상환자)에 대한 기준을 만족하는 데이터는 확인되지 않았다.
현재 진행 중인 여러 임상 시험이 있다. (see Supporting Appendix) 이러한 시험에서 단백질 선량은 차별화하고 동등한 에너지 섭취를 제공한다고 가정한다면 중증 환자에서 최적의 단백질 선량에 대해 더 깊은 이해를 할 수 있을 것이다.
3. In adult critically ill patients who are candidates for EN, does similar energy intake by PN vs EN as the primary feeding modality in the first week of critical illness impact clinical outcomes?
- There was no significant difference in clinical outcomes between early exclusive PN and EN during the first week of critical illness. As PN was not found to be superior to EN and no differences in harm were identified, we recommend that either PN or EN is acceptable.
ICU 입원 3일 이내 EN or PN을 시작하는 환자를 대상으로 무작위화하였다. 조기 PN과 EN을 비교한 대규모의 다기관 연구가 기준을 충족하였고 4798 명의 중환자가 선발되었다.
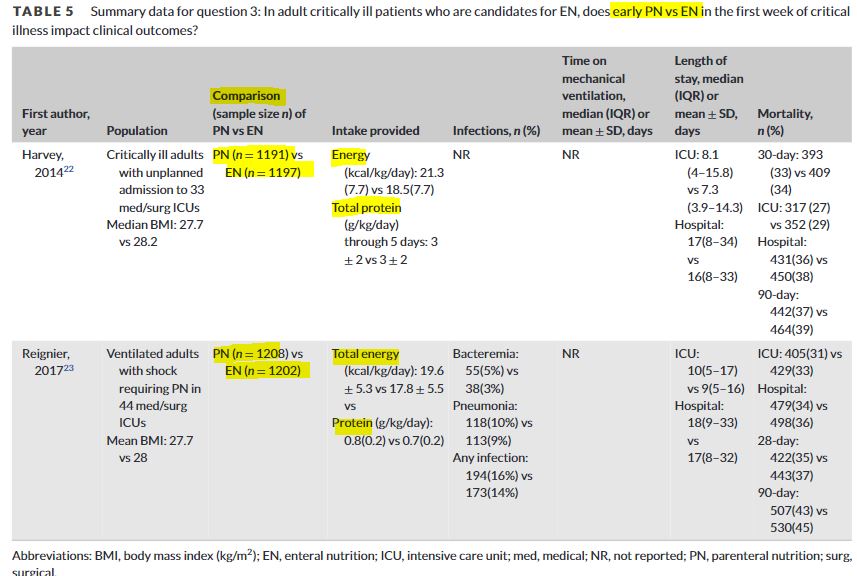
두 실험 모두 질문에 직접적으로 답변 가능하도록 고안되었고 연구 질이 높았다. 입원 후 36시간 이내 또는 삽관 후 24시간 이내 PN or EN 시작으로 무작위화 되었다. 개입 기간은 5-7일 밖에 되지 않았지만 보고된 결과는 무작위화에서부터 퇴원까지 추적 관찰하였으며 사망률은 퇴원 후 90일까지 추적되었다. 개입 기간 이외의 영양 섭취 정보는 제공되지 않았다.
The recommendation grade is strong, as there do not appear to be any harms or benefits concerning the choice of using EN vs PN. → EN vs PN에 따른 any harms or benefits에도 차이가 보이지 않았다. 이를 통해 EN or PN의 초기(in the first 1 week) 영양 경로 선택에 있어서 임상 결과의 차이보다는 비용 및 편의성이 더 큰 결정 요인이 될 것이다.
enteral feeding intolerance은 EN 군에서 더 흔하였다. PN의 초기 사용을 꺼렸던 이유 중의 하나는 바로 감염의 위험성 때문이었는데 early PN을 한다고 해서 감염이나 기타 부작용을 증가시키는 것은 발견되지 않았다.
2016 ASPEN-SCCM 가이드라인에서는 EN을 할 수 없는 환자에서 영양 위험이 낮은 경우 PN을 7일간 보류하되 영양 위험이 높은 경우 PN의 초기 사용을 권장하였다.
현재 지침에서는 보다 최근(2001-2020년), 보다 고품질의 대규모 다기관 임상 데이터를 기반을 기반으로 한다. 보다 최신의 영양 지원 관행(practice)을 통해 카테터 관리, 혈당 조절, overfeeding energy, 균혈증 등의 위험이 감소될 것으로 기대한다.
해당 권고안의 한계는 권고안의 기초가 되는 증거가 ICU 입원 첫 3일 이내 PN을 시작하여 5-7일 동안 PN을 유지하는 군을 대상(for a few days and not for weeks or longer)으로 한 임상이기 때문에 첫 주동안 EN을 할 수 없는 중환자가 조건이 된다. 따라서 복잡한 수술 등으로 인해 생기는 EN 불내성 환자로 일반화될 수 없을 수 있다.
4. In adult critically ill patients receiving early EN, does provision of SPN to meet energy targets vs no SPN during the first week of critical illness impact clinical outcomes?
- There was no significant difference in clinical outcomes. Based on findings of no clinically important benefit in providing SPN early in the ICU admission, we recommend not initiating SPN prior to day 7 of ICU admission.
* SPN, supplemental PN, 즉 EN을 하면서 부족한 칼로리를 채우기 위한 추가 PN(TPN 제형 포함)
Mean difference in bacteremia incidence in critically ill patients with supplemental parenteral nutrition (PN) vs no supplemental PN.
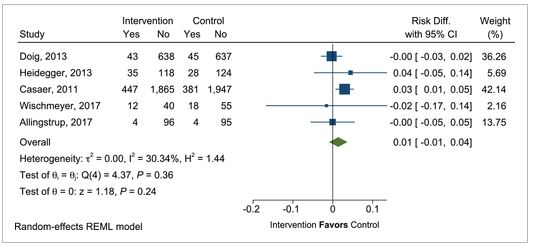
Mean difference in pneumonia incidence in critically ill patients with supplemental parenteral nutrition (PN) vs no supplemental PN.

Mean difference in intensive care unit mortality in critically ill patients with supplemental parenteral nutrition (PN) vs no supplemental PN.
이전 지침에서는 목표 단백질과 에너지 요구량의 60%가 충족되지 않을 때 7-10일 후 SPN을 사용할 것을 권고하였다. 2016년 지침에서는 SPN을 추가하기 위해 7-10일을 기다릴 것을 제안한 반면 포함된 임상 연구들은 3일째 SPN이 추가되었고 대부분 6-8일 동안 투여받았다. 그러나 감염 합병증이나 사망률의 차이가 발견되지 않았다. ICU 입원 초기 SPN을 제공함에도 불구하고 임상적으로 중요한 이점이 없다는 발견에 기초하여 입원 첫 7일 이내 SPN의 사용을 권장하지는 않는다.
ex) trial intervention
Patients were randomized to receive either EN (standard care) or SPN + EN. The type of enteral formula was selected by the individual treatment team following nutritional assessment. A standard polymeric solution with 1.2 ± 0.2 kcal/mL was used to standardize nutrition delivery. EN was initiated at 20 mL/hr and increased by 20 mL/hr increments every 4 hours as tolerated until the goal rate was reached. A bedside algorithm was developed to aid in initiating and progressing the EN rate.
In patients assigned to the SPN + EN group, all patients received SPN via central intravenous access and SPN administration began as soon as possible post-enrollment. We utilized a PN solution of similar caloric density to the standard EN solutions (1.2 kcals/mL, providing 0.06–0.09 g protein/mL). The PN solution utilized (OLIMEL N9, Baxter Inc., Deerfield, IL, USA) was a 1.1 kcal/mL solution—20% lipid (containing 80% olive oil and 20% soy oil), 27.5% glucose solution, and 14% amino acids. PN was initiated at 20 mL/hr and increased by 20 mL/hr increments every 4 hours as tolerated until 100% of goal calories were reached. The PN was adjusted daily to ensure that patients received 100% of their prescribed calories.
5A. In adult critically ill patients receiving PN, does provision of mixed-oil ILEs (ie, medium-chain triglycerides, olive oil, FO, mixtures of oils), as compared with 100% SO ILE, impact clinical outcomes?
- Owing to limited statistically or clinically significant differences in key outcomes, we suggest that either mixed-oil ILE or 100% SO ILE be provided to critically ill patients who are appropriate candidates for initiation of PN, including within the first week of ICU admission.
5B. In adult critically ill patients receiving PN, does provision of FO-containing ILE, as compared with non–FO-containing ILE, impact clinical outcomes?
- Because there was only one outcome with a significant difference that was not supported by data covering the other key downstream outcomes, we suggest that either FO- or non–FO-containing ILE be provided to critically ill patients who are appropriate candidates for initiation of PN, including within the first week of ICU admission.
reference:
1) Compher, Charlene, et al. "Guidelines for the provision of nutrition support therapy in the adult critically ill patient: The American Society for Parenteral and Enteral Nutrition." Journal of Parenteral and Enteral Nutrition (2021).
2) Wischmeyer, Paul E., et al. "A randomized trial of supplemental parenteral nutrition in underweight and overweight critically ill patients: the TOP-UP pilot trial." Critical care 21.1 (2017): 1-14.

댓글