😁 LMWH의 renal dosing 부분 (Lexicom)


😁 Ummhealth의 DVT 예방 프로토콜

😁 Comparison of published guidelines for management of coagulopathy and thrombosis in critically ill patients with COVID 19: implications for clinical practice and future investigations.
The CDC, ACCP, and ACF do not recommend therapeutic anticoagulation except in cases where there is a thromboembolic event or a high suspicion for a thromboembolic event when imaging is not possible. ASH recommends therapeutic anticoagulation only if there is a documented clinical indication (e.g., VTE, atrial fibrillation, or mechanical valve). ACC mentions that therapeutic anticoagulation is the key to VTE treatment but does not make a distinction between confirmed or suspected VTE. They do mention that hemodynamically stable patients with intermediate-low to intermediate-high risk PE should be managed initially with anticoagulation and close monitoring rather than fibrinolytics. While the SCC-ISTH recommends that therapeutic anticoagulation should not be considered for primary prevention until randomized trials are available, they do mention that therapeutic anticoagulation (i.e., changing from standard or intermediate intensity to therapeutic intensity) can be considered in patients without confirmed VTE but who have deteriorating pulmonary or ARDS. ASH also states that it is reasonable to consider increasing the intensity of the patient’s anticoagulation regimen (i.e., from standard to intermediate intensity, from intermediate to therapeutic intensity) or change anticoagulants in patients who have recurrent thrombosis of catheters and extracorporeal circuits (i.e., ECMO, CRRT) on prophylactic anticoagulation regimens. Similarly, the ACCP recommends increasing the dose of LMWH by 25–30% in patients with recurrent VTE despite being on therapeutic LMWH anticoagulation. The CDC specifically mentions that patients who have thrombosis of catheters or extracorporeal filters should be treated accordingly to standard institutional protocols for patients without COVID-19.
* Only the ACF recommends increasing the intensity of anticoagulation in critically ill patients (enoxaparin 40 mg twice daily or heparin 7500 unit/dose three times daily) while they recommend standard dose anticoagulant prophylaxis for all other hospitalized non-critically ill patients.
The ACC mentions that enoxaparin 40 mg daily or similar LMWH regimen (i.e., dalteparin 5000 u daily) can be administered with consideration of subcutaneous heparin (5000 u twice to three times per day) in patients with renal dysfunction (i.e., creatinine clearance < 30 mL/min).
😁 ACC: J Am Coll Cardiol. 2020 Jun, 75 (23) 2950–2973


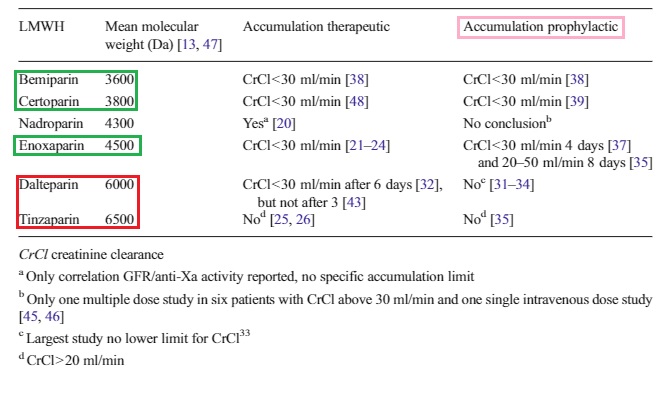
😁 A systematic review on the accumulation of prophylactic dosages of low-molecular-weight heparins (LMWHs) in patients with renal insufficiency
비록 대부분의 저분자량 헤파린(LMWHs)의 치료용량이 신부전 환자에게 축적되는 것으로 알려져 있지만, 예방용량은 이보다 저용량이기 때문에 이에 대한 축적 여부는 명확하게 입증되지 않았다. 그럼에도 불구하고, 종종 선량 감소가 권장된다. (ex. enoxaparin; CrCl<30 mL/min 일 때 30 mg q24h SC) 이번 연구에서는 신장 기능이 감소된 환자에게 LMWH의 예방적 투여량이 축적되는지 여부를 조사하기 위해 systematic review를 실시했다.
☞ 결과
- For dalteparin and tinzaparin, no accumulation was observed.
- Enoxaparin, on the other hand, did lead to accumulation in patients with renal insufficiency, although not in patients undergoing renal replacement therapy.
- Bemiparin and certoparin also did show accumulation.
- No data were available for nadroparin.
☞ 결론
- systematic review에서 신부전 환자에서 tinzaparin and dalteparin은 예방적 용량으로도 축적되지 않고 용량 감소 없이 안전할 가능성이 높았다.
- 하지만 enoxaparin, bemiparin, and certoparin의 경우 CrCl < 30 mL/min 에서 축적이 관찰되었으므로 감량이 필요하다. (cf. 놀랍게도 enoxaparin은 CVVH 환자나 혈액 투석 환자에서 축적을 보이지 않았다. 이는 신장 대체 요법에 의한 제거때문일 수 있다)
- 축적 여부의 차이는 아마도 LMWH의 분자량 차이일지도 모른다. 분자량이 클 수록 신장 청소율에 덜 의존한다.
☞ LMWH vs UFH
- 적어도 VTE의 예방과 치료에 있어 LMWH은 UFH과 동등하게 효과적이며 정기적인 실험실적 모니터링 없이 투여가 가능하다.
- 뿐만 아니라 보다 예측 가능한 항응고 반응, 더 긴 반감기(1일 1-2회 투여), dose-independent elimination 및 헤파린 유도 혈소판 감소증을 덜 유발한다는 장점을 가지고 있다.
- 주요 출혈 발생에 대한 상반되는 증거가 있긴 하지만 코크란 연구(Cochrane analysis)애서는 UFH에 비해 주요 출혈 발생율이 낮았다.
1) Dalteparin
- 총 157명의 환자를 대상으로 6일 또는 10일 차의 peak anti-Xa activity에서 축적의 근거를 찾지 못했다.
- 총 157명의 CVVH를 받지 않는 ICU 환자에서 9일 또는 12일 차의 trough와 peak anti-Xa activity에서 축적의 근거를 찾지 못했다.
- 혈액 투석하는 7명의 환자를 대상으로 2500 IU dapteparin을 4주동안 투여하였을 때 anti-Xa acitivity는 1주차 또는 4주차 때, 시간(1, 2, 3, 4, 24, and 28 h post-injection)에 따라 큰 차이가 없었다.
2) Enoxaparin
Three studies of which two in patients older than 75 years examined enoxaparin accumulation in, respectively, 125, 28, and 48 non-dialysis patients. The studies in the elderly with CrCl 20–50 ml/min found a significantly higher maximum concentration (Cmax), area under the curve (AUC), and trough anti-Xa activity (24 h postinjection) after 8 days administration and a higher peak anti-Xa activity after 10 days, compared to patients with better renal function. The other study in patients with different severity of renal insufficiency found accumulation (a significantly higher Cmax, longer half-life, higher AUC) already on day 4 in patients with CrCl ≤ 30 ml/min.
Hemodialysis patients (n = 7) prescribed 40 mg enoxaparin at hemodialysis sessions for 4 weeks, anti-Xa activity at different time points postinjection were not significantly different between week 1 and week 4. Also in ICU patients (n = 12) undergoing CVVH with a flow rate of 30 ml/kg/h, no accumulation of enoxaparin (30 mg daily) was found.
reference:
1) Lexicomp
2) Flaczyk, Adam, et al. "Comparison of published guidelines for management of coagulopathy and thrombosis in critically ill patients with COVID 19: implications for clinical practice and future investigations." Critical Care 24.1 (2020): 1-13.
3) Atiq, Ferdows, et al. "A systematic review on the accumulation of prophylactic dosages of low-molecular-weight heparins (LMWHs) in patients with renal insufficiency." European journal of clinical pharmacology 71.8 (2015): 921-929.
'🤹♂️ 카테고리별 약물 > 심혈관' 카테고리의 다른 글
| isosorbide-5-mononitrate vs isosorbide dinitrate: ISMN와 ISDN의 차이 (0) | 2021.08.24 |
|---|---|
| Aspirin: Recovery time, Turnover platelet, 위장관 출혈 부작용 (0) | 2021.08.03 |
| 쿠스토디올 액: 개심술 수액, open heart, 심정지액 (0) | 2021.07.17 |
| 칼슘채널 차단제(Calcium channel blocker; CCB) 약제 별 차이: L type CCB vs T type CCB (0) | 2021.07.13 |
| VTE(venous thromboembolism) CHEST 2016 guideline: 하지심부정맥혈전증, 폐색전증 치료 (0) | 2021.06.23 |

댓글